

Cryoablation for Palliation of Painful Bone Metastases: The MOTION Multicenter Study
- PMID: 33817650
- PMCID: PMC8011449
- DOI: 10.1148/rycan.2021200101
Cryoablation for Palliation of Painful Bone Metastases: The MOTION Multicenter Study
Abstract
Purpose: To assess the clinical effectiveness of cryoablation for palliation of painful bone metastases.
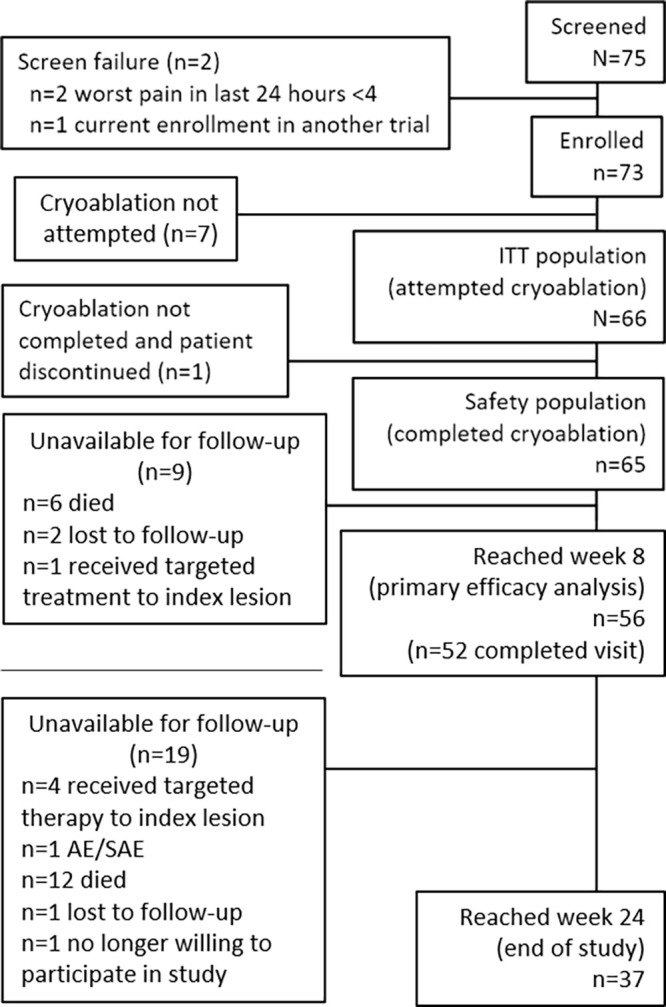
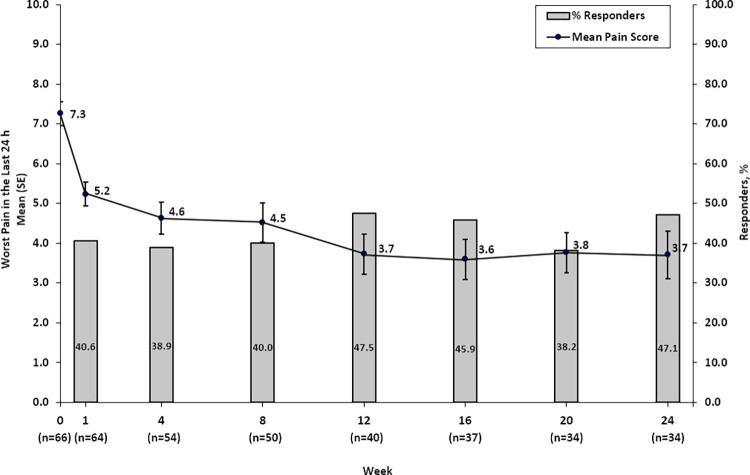
Materials and methods: MOTION (Multicenter Study of Cryoablation for Palliation of Painful Bone Metastases) (ClinicalTrials.gov NCT02511678) was a multicenter, prospective, single-arm study of adults with metastatic bone disease who were not candidates for or had not benefited from standard therapy, that took place from February 2016 to March 2018. At baseline, participants rated their pain using the Brief Pain Inventory-Short Form (reference range from 0 to 10 points); those with moderate to severe pain, who had at least one metastatic candidate tumor for ablation, were included. The primary effectiveness endpoint was change in pain score from baseline to week 8. Participants were followed for 24 weeks after treatment. Statistical analyses included descriptive statistics and logistic regression to evaluate changes in pain score over the postprocedure follow-up period.
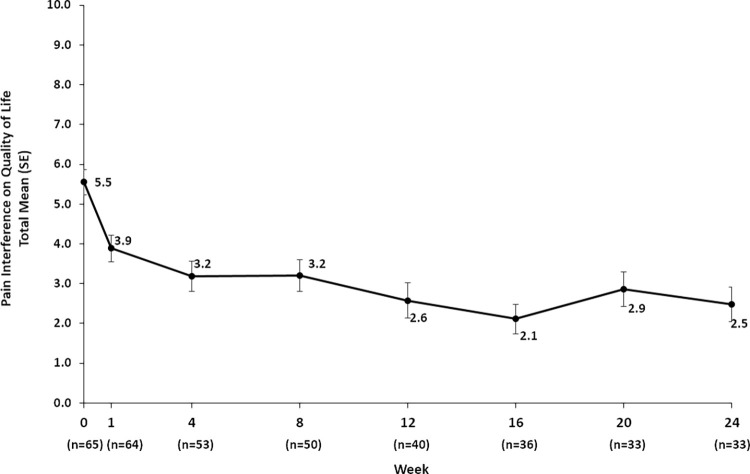
Results: A total of 66 participants (mean age, 60.8 years ± 14.3 [standard deviation]; 35 [53.0%] men) were enrolled and received cryoablation; 65 completed follow-up. Mean change in pain score from baseline to week 8 was -2.61 points (95% CI: -3.45, -1.78). Mean pain scores improved by 2 points at week 1 and reached clinically meaningful levels (more than a 2-point decrease) after week 8; scores continued to improve throughout follow-up. Quality of life improved, opioid doses were stabilized, and functional status was maintained over 6 months. Serious adverse events occurred in three participants.
Conclusion: Cryoablation of metastatic bone tumors provided rapid and durable pain palliation, improved quality of life, and offered an alternative to opioids for pain control.Keywords: Ablation Techniques, Metastases, Pain Management, Radiation Therapy/OncologySupplemental material is available for this article.© RSNA, 2021.
Keywords: Ablation Techniques; Metastases; Pain Management; Radiation Therapy/Oncology.
2021 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: J.W.J. Activities related to the present article: disclosed grant to author’s institution from Washington University for study support for data collection and cryoprobes for ablation; author received consultancy fees from Galil Medical and BTG regarding development of a microwave device, not related to cryoablation; Galil Medical and BTG provided cryoprobes for the study and assistance with manuscript, including graphs and tables. Activities not related to the present article: author received consultancy fees from Bard, Merit Medical, and Stryker. Other relationships: disclosed no relevant relationships. J.D.P. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author received consultancy fees from Galil Medical and BTG; author’s institution is a study grant recipient from Galil Medical and BTG for an investigator-initiated study. Other relationships: author’s institution has patents pending from Focused Cryo involving a new cryoablation device. J.G. Activities related to the present article: author received fees from BTG and Galil for participation in review activities. Activities not related to the present article: author received payment for lectures including service on speakers bureaus from Canon, J&J, Medtronic, and BTG. Other relationships: disclosed no relevant relationships. A.G. disclosed no relevant relationships. X.B. disclosed no relevant relationships. J.P. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: disclosed consultancy fees paid to author’s institution from Boston Scientific; disclosed money paid to author from Philips for development of educational presentations. Other relationships: disclosed no relevant relationships. A.N.K. Activities related to the present article: disclosed grant to author’s institution from Galil Medical as sponsor for this trial. Activities not related to the present article: disclosed grants/grants pending to author’s institution from Philips and EDDA Technology; author received royalties from UpToDate. Other relationships: disclosed no relevant relationships. M.C. Activities related to the present article: author’s institution received grant from Galil Medical; author received consultancy fees or honorarium from Medtronic and Varian. Activities not related to the present article: disclosed no relevant relationships. Other relationships: disclosed no relevant relationships. S.G. disclosed no relevant relationships. F.A. Activities related to the present article: author’s institution participated in MOTION clinical trial and received expenses from Galil as per study protocol. Activities not related to the present article: disclosed no relevant relationships. Other relationships: disclosed no relevant relationships. A.J.H. disclosed no relevant relationships. J.I. disclosed no relevant relationships. F.P. disclosed no relevant relationships. C.M. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author received consultancy fees from Deeplink Medical. Other relationships: disclosed no relevant relationships. P.J.L. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author received honoraria and support for travel to meetings from Endocare and Galil Medical for invited talks on cryoablation, not related to the trial or associated data. Other relationships: disclosed no relevant relationships. T.d.B. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author received consultancy fees from Terumo and Guerbet; author’s institution has grants/grants pending from Terumo; author received payment for lectures including service on speakers bureaus from Guerbet, Boston Scientific, Terumo, AstraZeneca, GE Healthcare, and Nanobiotix. Other relationships: disclosed no relevant relationships. F.D. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author received consultancy fees from Medtronics, Ablatech, GE, Galil Medical, and Terumo. Other relationships: disclosed no relevant relationships.
Figures




References
-
- Janssen SJ, Pereira NRP, Thio QCBS, et al. Physical function and pain intensity in patients with metastatic bone disease. J Surg Oncol 2019;120(3):376–381. - PubMed
-
- von Moos R, Costa L, Ripamonti CI, Niepel D, Santini D. Improving quality of life in patients with advanced cancer: Targeting metastatic bone pain. Eur J Cancer 2017;71:80–94. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
