

Abdominal elastotic lesions. A clinicopathologic study of 23 cases
- PMID: 33817725
- PMCID: PMC8112749
- DOI: 10.47162/RJME.61.3.22
Abdominal elastotic lesions. A clinicopathologic study of 23 cases
Abstract
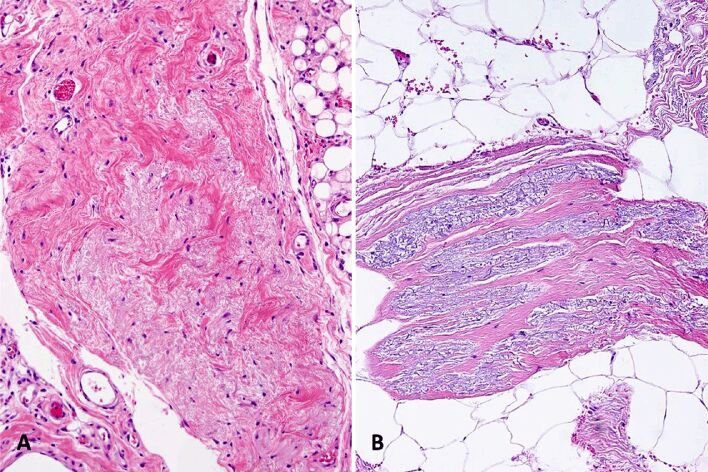
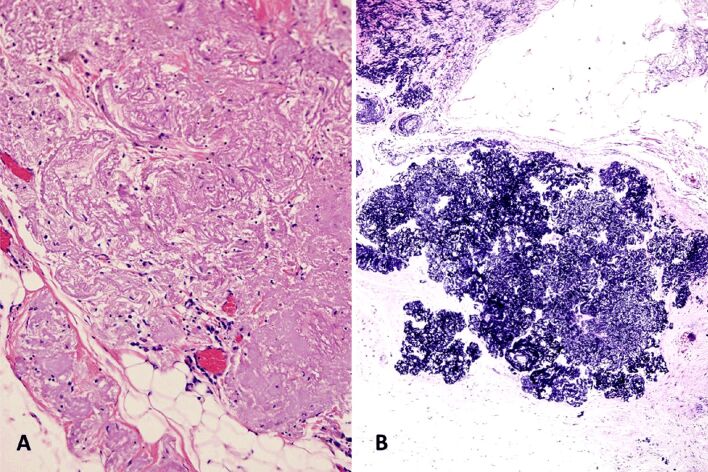
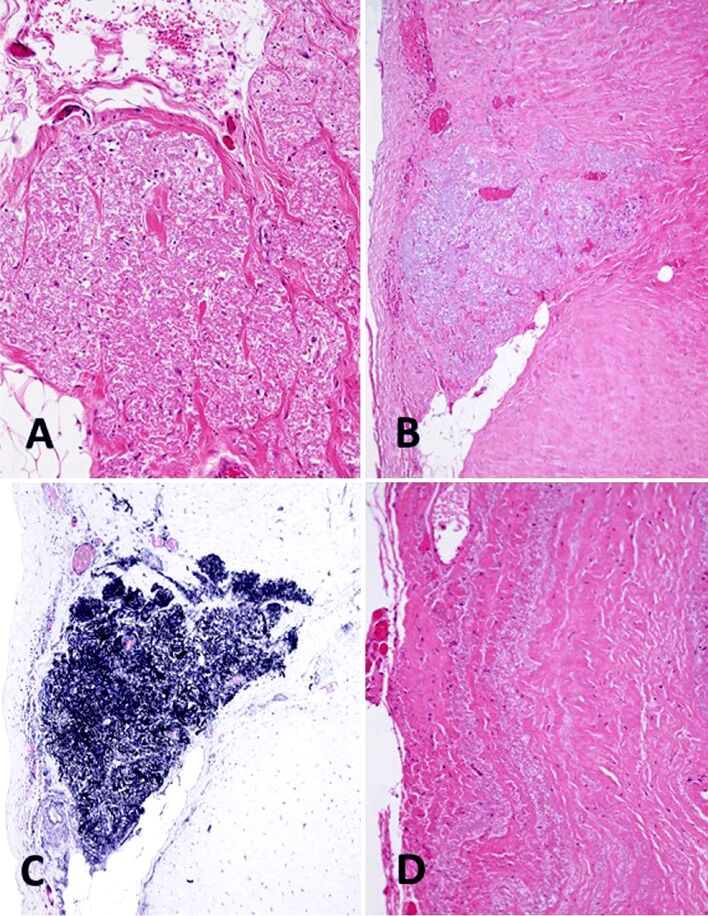
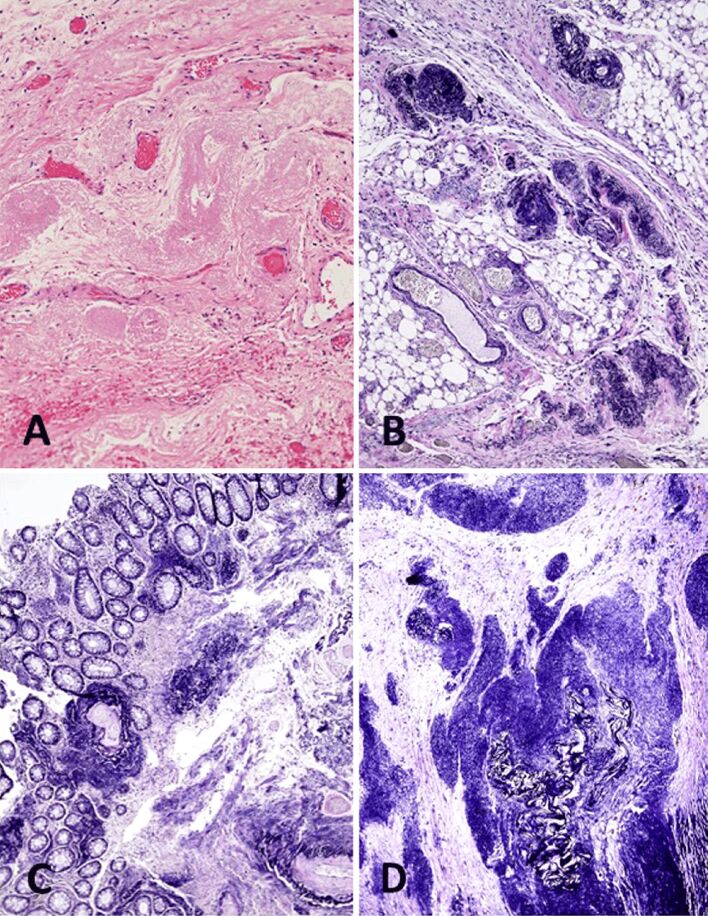
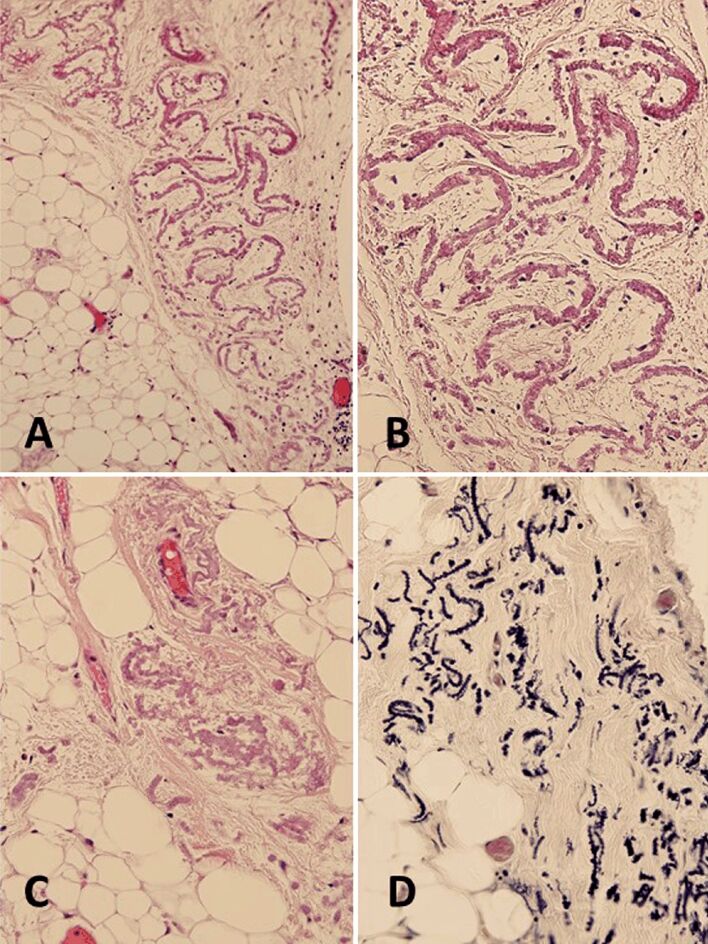
Abdominal elastotic deposits are uncommon lesions that often presents as polyps. They show three histological patterns: fibroelastosis, angioelastosis, and elastofibroma. We describe 23 cases including rare locations, such as mesentery, greater omentum, hernia sac, spleen, peripancreatic fat, and hypodermal fat. The age of the patients ranged from 49 to 93 years (mean, 76.8 years). Most lesions were discovered incidentally in the microscopic study. The most frequent locations were peritoneal subserosa (43.5%) and mesentery∕mesocolon∕greater omentum (39.1%). The most common pattern was fibroelastosis (69.6%) followed by angioelastosis (26.1%). We observed one case of omental elastofibroma. A review of the 14 abdominal elastofibromas described including our case revealed that the age of the patients ranged from 45 to 88 years (mean, 68.5 years). Female predominance is striking (M:F, 1:12). The most common site was the stomach (50%). The greater omentum (14.3%), small intestine (7.1%), and pancreas (7.1%) are very rare sites for this lesion. Only one case before ours has been published in the greater omentum. The size of the lesions ranged from 0.7 cm to 8 cm (mean 3.2 cm). In 36.4% of the cases located in the digestive tract, the mucosa did not show alterations. Ulcerations (36.4%) or polypoid excrescences (18.2%) were mostly observed. Six (42.9%) cases were asymptomatic and six (42.9%) cases simulated a neoplasm. Two cases were associated with elastofibromas in other locations. Differential diagnosis includes amyloidoma, elastofibrolipoma, mesenteric elastic vascular sclerosis in neuroendocrine tumors, diverticular disease elastosis, pseudoxanthoma elasticum, pulse granuloma, and digestive lesions in patients treated with D-Penicillamine.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures

Similar articles
-
Reactive nodular fibrous pseudotumor of the gastrointestinal tract and mesentery: a clinicopathologic study of five cases.Am J Surg Pathol. 2003 Apr;27(4):532-40. doi: 10.1097/00000478-200304000-00015. Am J Surg Pathol. 2003. PMID: 12657940
-
Gastrointestinal stromal tumors presenting as omental masses--a clinicopathologic analysis of 95 cases.Am J Surg Pathol. 2009 Sep;33(9):1267-75. doi: 10.1097/PAS.0b013e3181a13e99. Am J Surg Pathol. 2009. PMID: 19440146
-
Well-differentiated papillary mesothelioma of the female peritoneum: a clinicopathologic study of 26 cases.Am J Surg Pathol. 2012 Jan;36(1):117-27. doi: 10.1097/PAS.0b013e3182354a79. Am J Surg Pathol. 2012. PMID: 22024662
-
Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature.Am J Surg Pathol. 2005 Dec;29(12):1558-75. doi: 10.1097/01.pas.0000173232.22117.37. Am J Surg Pathol. 2005. PMID: 16327428 Review.
-
CT of the mesentery, omentum, and peritoneum in children.Radiographics. 1995 Jan;15(1):89-104. doi: 10.1148/radiographics.15.1.7899616. Radiographics. 1995. PMID: 7899616 Review.
References
-
- Kharsa G, Molas G, Potet F, Baglin AC, Vaury P, Grossin M. Élastomes du côlon. Discussion pathogénique à propos de 7 observations [Colonic elastoma. A pathologic study of 7 cases] Ann Pathol. 1992;12(6):362–366. - PubMed
-
- Hobbs CM, Burch DM, Sobin LH. Elastosis and elastofibromatous change in the gastrointestinal tract: a clinicopathologic study of 13 cases and a review of the literature. Am J Clin Pathol. 2004;122(2):232–237. - PubMed
-
- Märkl B, Kerwel TG, Langer E, Müller W, Probst A, Spatz H, Arnholdt HM. Elastosis of the colon and the ileum as polyp causing lesions: a study of six cases and review of the literature. Pathol Res Pract. 2008;204(6):395–399. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
