

Pulmonary Embolism Response Team utilization during the COVID-19 pandemic
- PMID: 33818200
- PMCID: PMC8047511
- DOI: 10.1177/1358863X21995896
Pulmonary Embolism Response Team utilization during the COVID-19 pandemic
Abstract
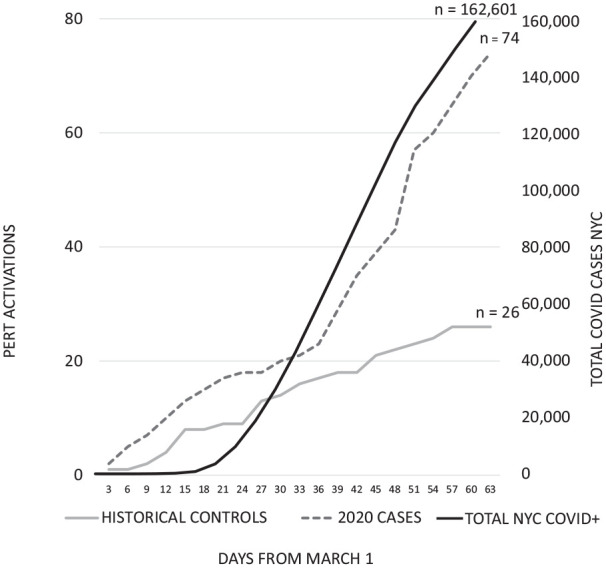
Coronavirus disease 2019 (COVID-19) may predispose patients to venous thromboembolism (VTE). Limited data are available on the utilization of the Pulmonary Embolism Response Team (PERT) in the setting of the COVID-19 global pandemic. We performed a single-center study to evaluate treatment, mortality, and bleeding outcomes in patients who received PERT consultations in March and April 2020, compared to historical controls from the same period in 2019. Clinical data were abstracted from the electronic medical record. The primary study endpoints were inpatient mortality and GUSTO moderate-to-severe bleeding. The frequency of PERT utilization was nearly threefold higher during March and April 2020 (n = 74) compared to the same period in 2019 (n = 26). During the COVID-19 pandemic, there was significantly less PERT-guided invasive treatment (5.5% vs 23.1%, p = 0.02) with a numerical but not statistically significant trend toward an increase in the use of systemic fibrinolytic therapy (13.5% vs 3.9%, p = 0.3). There were nonsignificant trends toward higher in-hospital mortality or moderate-to-severe bleeding in patients receiving PERT consultations during the COVID-19 period compared to historical controls (mortality 14.9% vs 3.9%, p = 0.18 and moderate-to-severe bleeding 35.1% vs 19.2%, p = 0.13). In conclusion, PERT utilization was nearly threefold higher during the COVID-19 pandemic than during the historical control period. Among patients evaluated by PERT, in-hospital mortality or moderate-to-severe bleeding were not significantly different, despite being numerically higher, while invasive therapy was utilized less frequently during the COVID-19 pandemic.
Keywords: COVID-19; SARS-CoV-2; pulmonary embolism response team (PERT); venous thromboembolism.
Conflict of interest statement
Figures


Comment in
-
PERTinent new insights into venous thromboembolism risk and management in hospitalized patients with COVID-19.Vasc Med. 2021 Aug;26(4):434-436. doi: 10.1177/1358863X211012776. Epub 2021 May 20. Vasc Med. 2021. PMID: 34014133 No abstract available.
References
-
- Stam HJ, Stucki G, Bickenbach J.Covid-19 and post intensive care syndrome: A call for action. J Rehabil Med 2020; 52: jrm00044. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
