

Assessment of Patient-Preferred Language to Achieve Goal-Aligned Deprescribing in Older Adults
- PMID: 33818621
- PMCID: PMC8022217
- DOI: 10.1001/jamanetworkopen.2021.2633
Assessment of Patient-Preferred Language to Achieve Goal-Aligned Deprescribing in Older Adults
Abstract
Importance: How clinicians communicate about deprescribing, the structured process of reducing or stopping unnecessary, potentially harmful, or goal-discordant medicines, may be associated with the extent to which older adults are willing to do it.
Objective: To examine older adults' preferences regarding different rationales a clinician may use to explain why a patient should stop an unnecessary or potentially harmful medication.
Design, setting, and participants: This cross-sectional survey study was conducted from March 25 to April 19, 2020, among a nationally representative, probability-based online survey panel (KnowledgePanel). KnowledgePanel members aged 65 years and older were recruited by random digit dialing and address-based sampling. Data were analyzed from May 4 to July 8, 2020.
Exposures: The survey presented 2 vignettes involving hypothetical older adults. One described a statin being used for primary prevention by a person with functional impairment and polypharmacy. The second described a sedative-hypnotic, such as zolpidem, being used for insomnia by a person with good functional status.
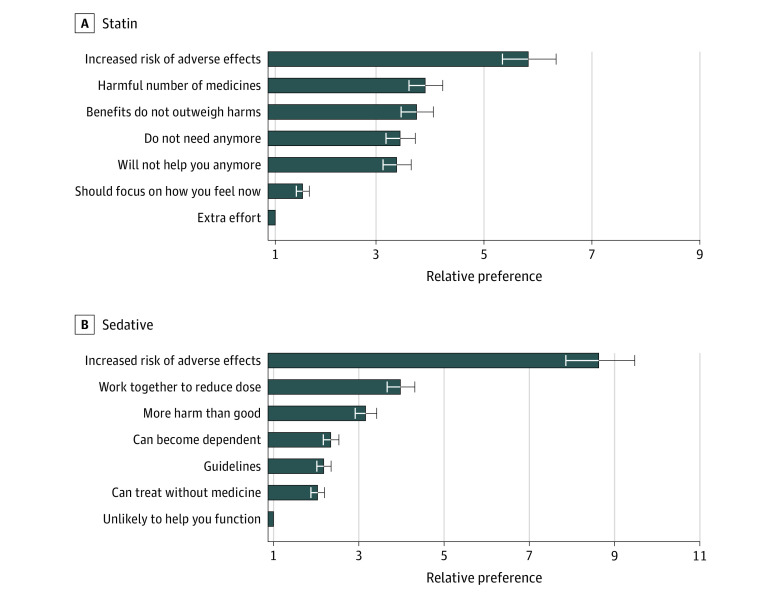
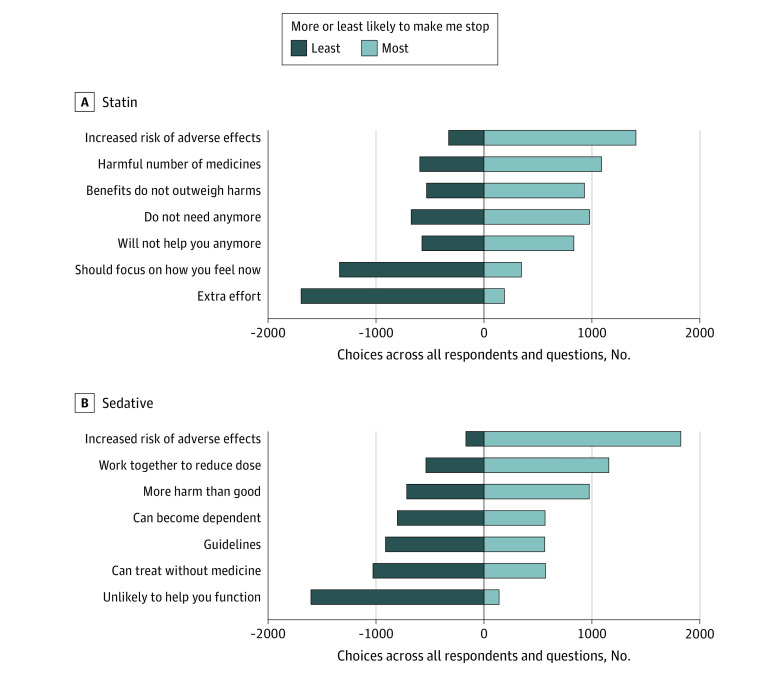
Main outcomes and measures: After each vignette, participants expressed preferences using a best-worst scaling method for 7 different phrases a clinician may use to explain why they should reduce or stop the medication. Conditional logistic regression was used to quantify respondents' relative preferences.
Results: A total of 1193 KnowledgePanel members were invited, and 835 respondents (70.0%) completed the survey. The mean (SD) age was 73 (6) years, 414 (49.6%) were women, and 671 (80.4%) self-identified as White individuals. A total of 496 respondents (59.8%) had ever used a statin, and 124 respondents (14.9%) had ever used a sedative-hypnotic. For both medications, the most preferred phrase to explain deprescribing focused on the risk of side effects. For statins, this phrase was 5.8-fold (95% CI, 5.3-6.3) more preferred than the least preferred option, which focused on the effort (treatment burden) involved in taking the medicine. For sedative-hypnotics, the phrase about side effects was 8.6-fold (95% CI, 7.9-9.5) more preferred over the least preferred option, "This medicine is unlikely to help you function better."
Conclusions and relevance: These findings suggest that among older adults, the most preferred rationale for deprescribing both preventive and symptom-relief medicines focused on the risk of side effects. These results could be used to inform clinical practice and improve effective communications around deprescribing in older adults.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
