

Clinical Burden of Concomitant Joint Disease in Psoriasis: A US-Linked Claims and Electronic Health Records Database Analysis
- PMID: 33818686
- PMCID: PMC8107168
- DOI: 10.1007/s12325-021-01698-7
Clinical Burden of Concomitant Joint Disease in Psoriasis: A US-Linked Claims and Electronic Health Records Database Analysis
Abstract
Background: Few studies have evaluated the clinical burden of concomitant joint disease in patients with psoriasis (PSO). The objective of this study was to assess comorbidity rates in patients with psoriatic arthritis (PsA) compared with PSO alone.
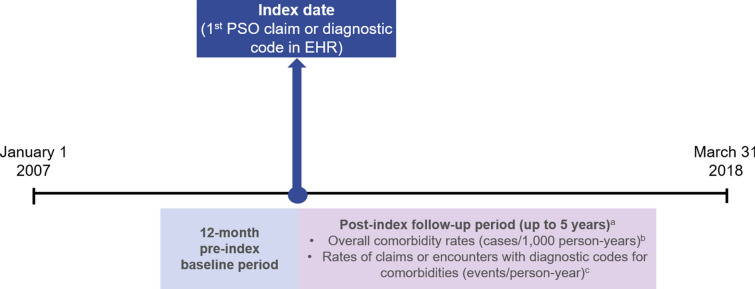
Methods: This was a retrospective study of US patients with prevalent PSO. Linked medical claims and electronic health records (EHR) in Optum's de-identified Integrated Claims-Clinical dataset were analyzed from 2007 to 2018. Patients were followed for up to 5 years after the first claim/diagnostic code for PSO (index date). Baseline comorbidity prevalence and follow-up rates (cases per 1000 person-years) were assessed using descriptive statistics. Comorbidity rate analysis included patients with the respective comorbidity at baseline.
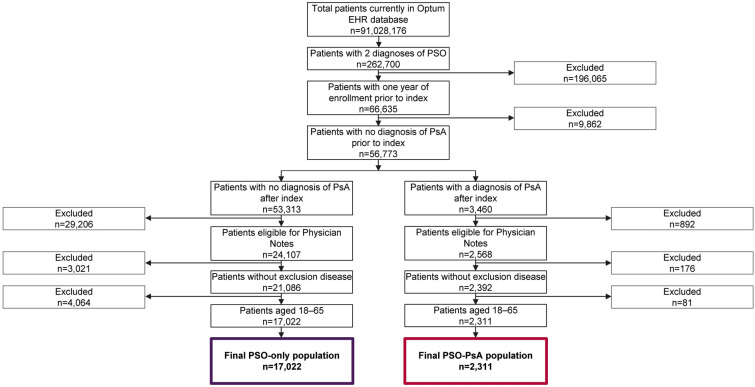
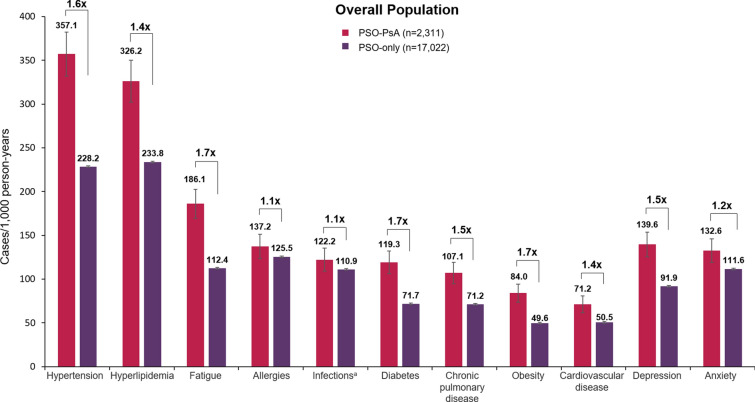
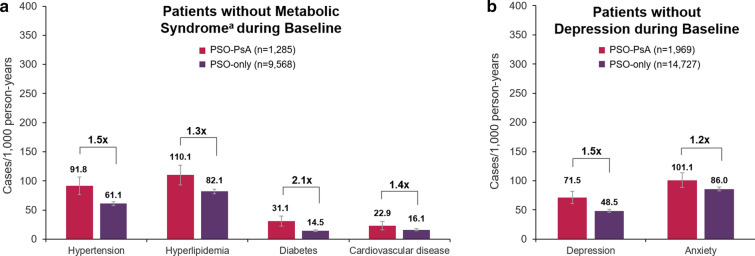
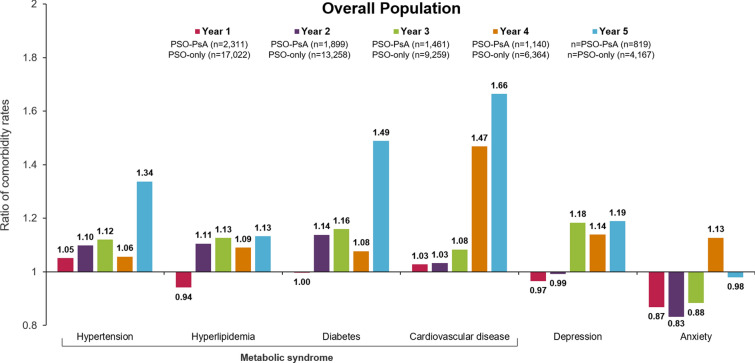
Results: Baseline demographics and comorbidity prevalence were numerically similar between patients with concomitant joint disease (PSO-PsA) and those with PSO alone (PSO-only). During follow-up, comorbidity rates were higher in patients in the PSO-PsA group than patients in the PSO-only group. Ratios of PSO-PsA comorbidity rates relative to PSO-only ranged from 1.1 for allergies and infections to 1.7 for fatigue, diabetes, and obesity. Comorbidity rate ratios increased from year 1 to year 5 for hypertension (1.05-1.34), hyperlipidemia (0.94-1.13), diabetes (1.00-1.49), cardiovascular disease (1.03-1.66), depression (0.97-1.19), and anxiety (0.87-0.98).
Conclusions: Patients with PsA have a larger clinical burden, characterized by higher comorbidity rates, than those with PSO. Future research should explore PsA risk factors and how physicians can monitor and treat patients with PSO to reduce the risk of PsA and the associated clinical burden.
Keywords: Claims; Comorbidities; Electronic health records; Psoriasis; Psoriatic arthritis.
Plain language summary
Psoriasis is a disease that causes scaly, red skin patches that are itchy or painful. About one-third of people who have psoriasis also develop joint pain. This combination of skin symptoms and joint disease is known as psoriatic arthritis. Having psoriatic arthritis can have a greater effect on people’s quality of life than having psoriasis alone. People with psoriasis or psoriatic arthritis often have other medical conditions that are not related to their skin or joints. We know that some conditions, such as obesity and high blood pressure, are more common in people with psoriatic arthritis than in those who only have psoriasis. However, more evidence is needed to understand if this pattern is also seen with other medical conditions. We used a large database of medical insurance claims and electronic health records to see what other medical conditions people with psoriatic arthritis or psoriasis had. We found that people with psoriatic arthritis were more likely to have other medical conditions than those with only psoriasis, including high blood pressure, obesity, diabetes, heart disease, and mental health conditions. These differences became larger over the years covered by this study (2007–2018). The results of this study show that people with psoriatic arthritis are more likely to have additional medical conditions than those who have psoriasis alone. Therefore, it is very important that doctors understand how to reduce the risk of joint disease in their patients with psoriasis.
Figures
References
-
- Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512–516. - PubMed
-
- Feldman SR, Hur P, Zhao Y, et al. Incidence rates of comorbidities among patients with psoriasis in the United States. Dermatol Online J. 2018;24(10):13030/qt2m18n6vj. - PubMed
-
- Ungprasert P, Srivali N, Thongprayoon C. Association between psoriasis and chronic obstructive pulmonary disease: a systematic review and meta-analysis. J Dermatol Treat. 2016;27(4):316–321. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
