

Recipient pre-existing chronic hypotension is associated with delayed graft function and inferior graft survival in kidney transplantation from elderly donors
- PMID: 33819285
- PMCID: PMC8021200
- DOI: 10.1371/journal.pone.0249552
Recipient pre-existing chronic hypotension is associated with delayed graft function and inferior graft survival in kidney transplantation from elderly donors
Abstract
Background: Pre-existing chronic hypotension affects a percentage of kidney transplanted patients (KTs). Although a relationship with delayed graft function (DGF) has been hypothesized, available data are still scarce and inconclusive.
Methods: A monocentric retrospective observational study was performed on 1127 consecutive KTs from brain death donors over 11 years (2003-2013), classified according to their pre-transplant Mean Blood Pressure (MBP) as hypotensive (MBP < 80 mmHg) or normal-hypertensive (MBP ≥ 80 mmHg, with or without effective antihypertensive therapy).
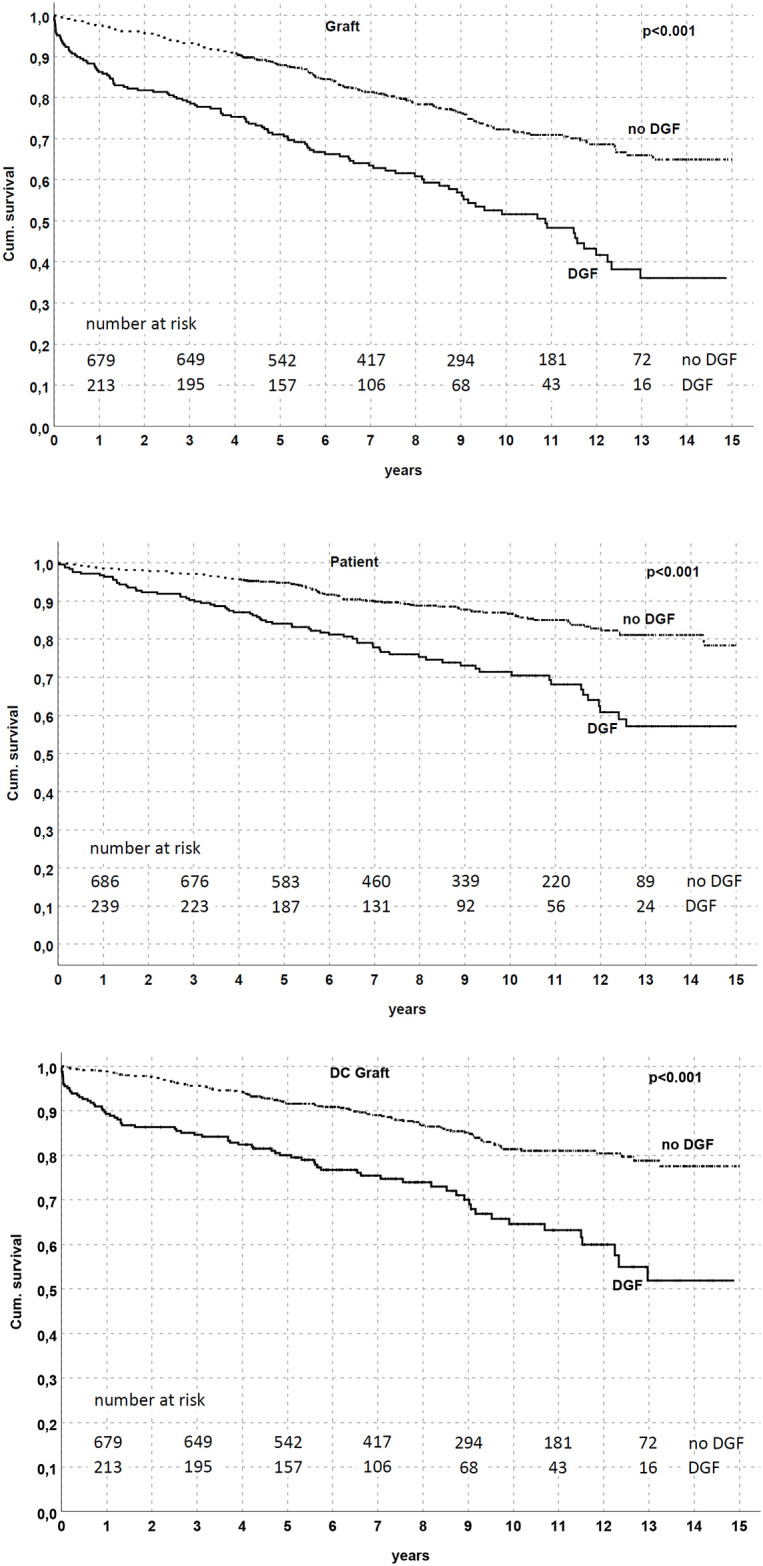
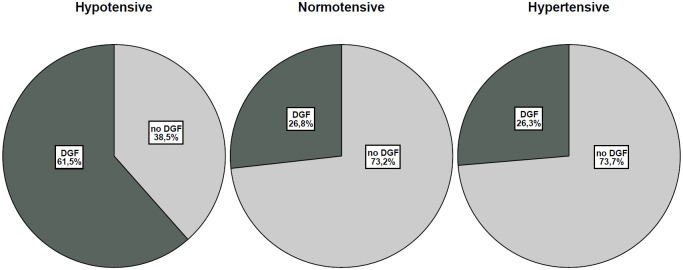
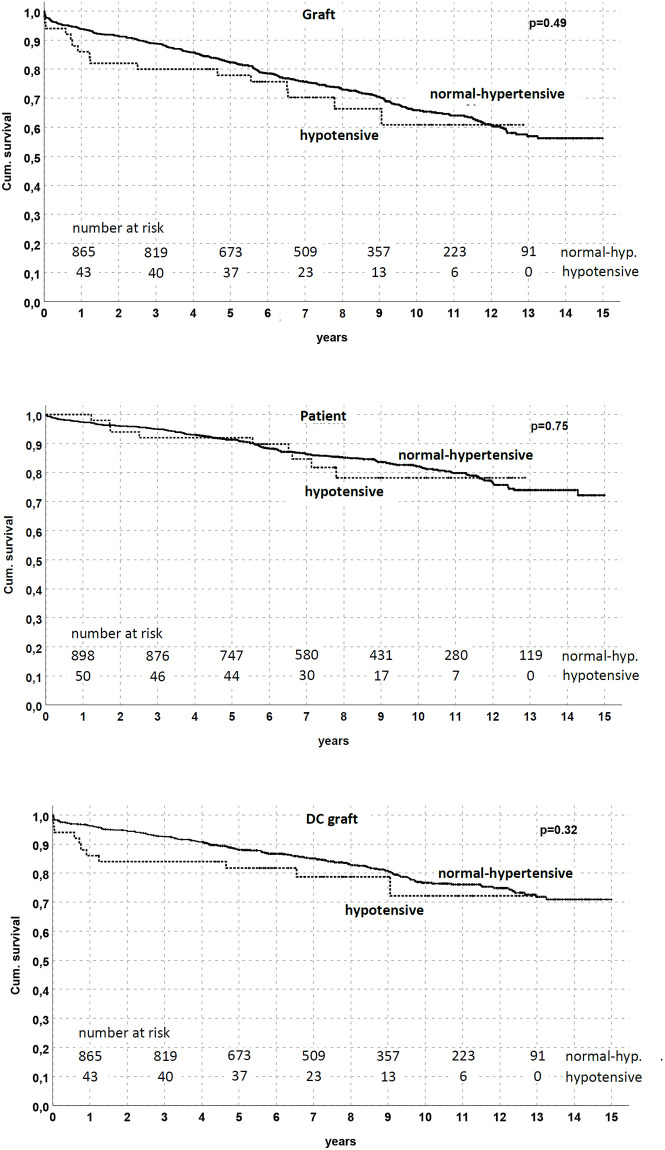
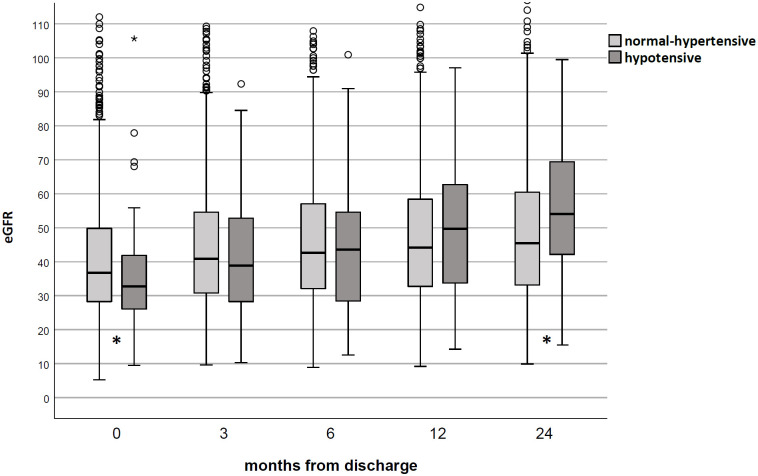
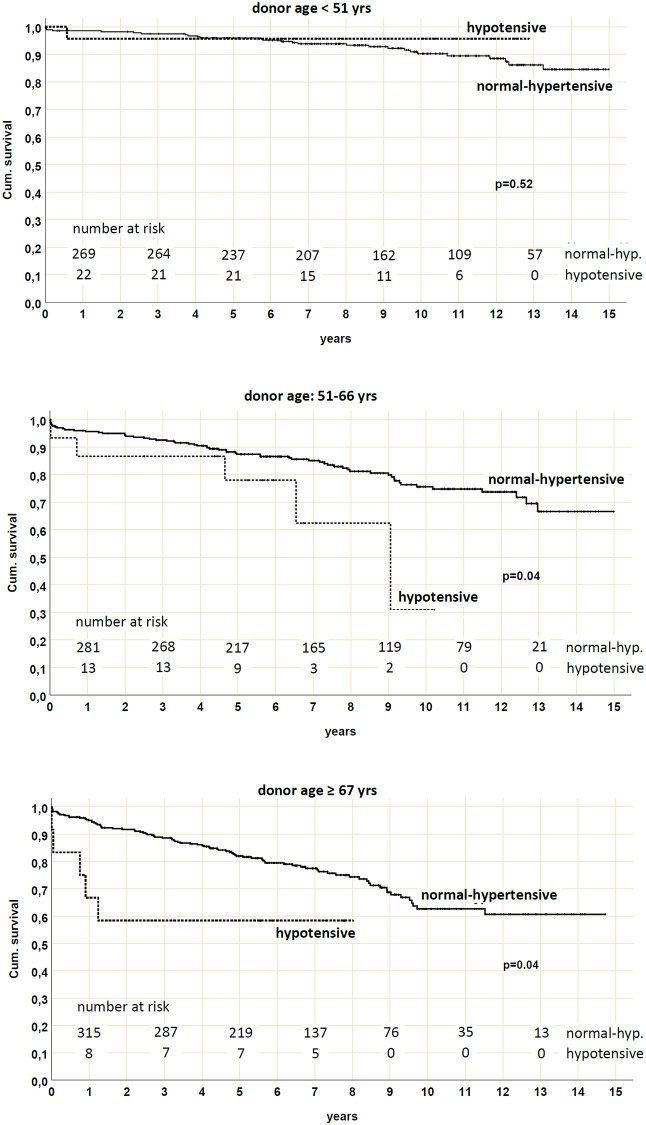
Results: Univariate analysis showed that a pre-existing hypotension is associated to DGF occurrence (p<0.01; OR for KTs with MBP < 80 mmHg, 4.5; 95% confidence interval [CI], 2.7 to 7.5). Chronic hypotension remained a major predictive factor for DGF development in the logistic regression model adjusted for all DGF determinants. Adjunctive evaluations on paired grafts performed in two different recipients (one hypotensive and the other one normal-hypertensive) confirmed this assumption. Although graft survival was only associated with DGF but not with chronic hypotension in the overall population, stratification according to donor age revealed that death-censored graft survival was significantly lower in hypotensive patients who received a KT from >50 years old donor.
Conclusions: Our findings suggest that pre-existing recipient hypotension, and the subsequent hypotension-related DGF, could be considered a significant detrimental factor, especially when elderly donors are involved in the transplant procedure.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
