

A Liquid Biopsy Assay for Noninvasive Identification of Lymph Node Metastases in T1 Colorectal Cancer
- PMID: 33819484
- PMCID: PMC10360659
- DOI: 10.1053/j.gastro.2021.03.062
A Liquid Biopsy Assay for Noninvasive Identification of Lymph Node Metastases in T1 Colorectal Cancer
Abstract
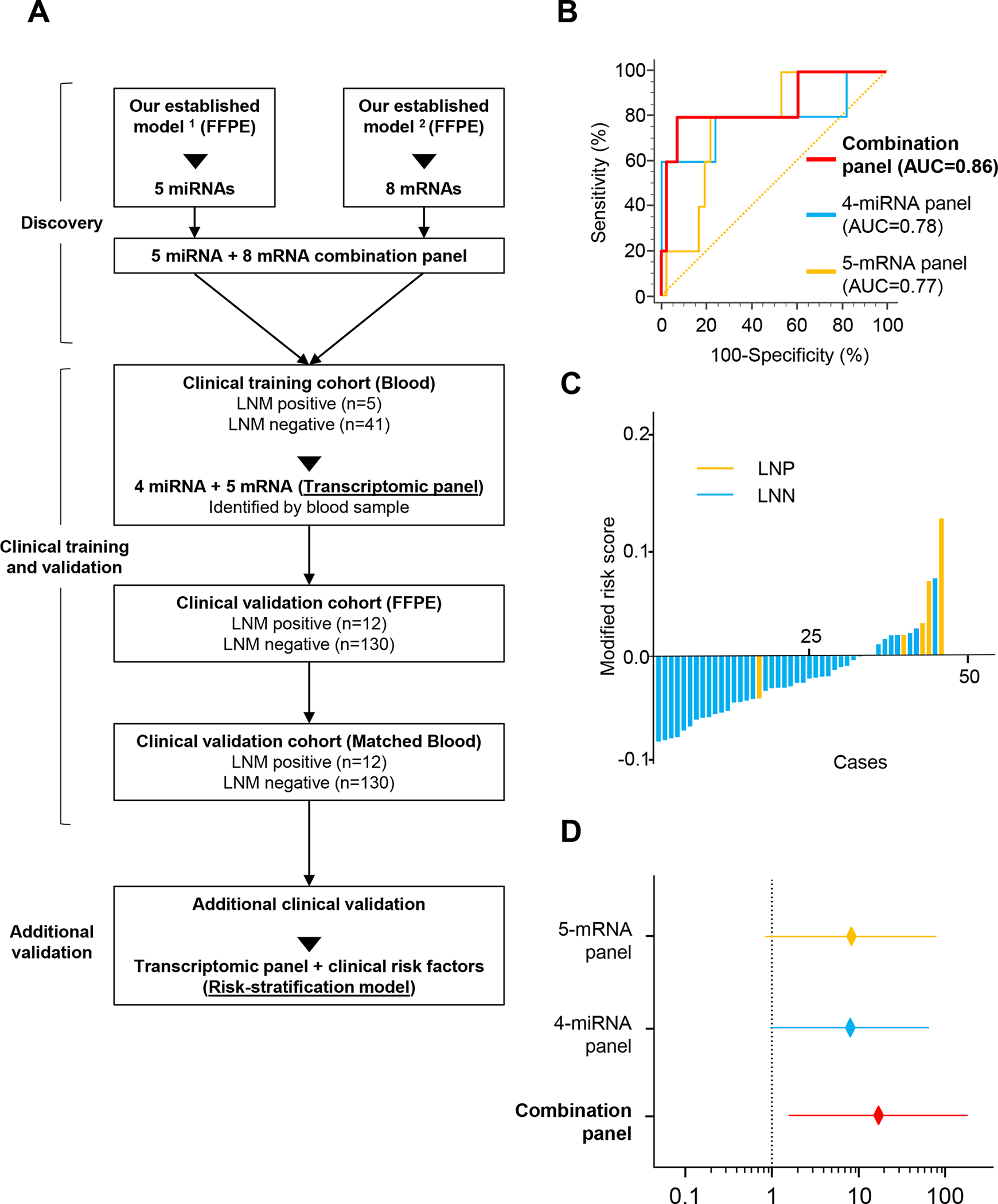
Background & aims: We recently reported use of tissue-based transcriptomic biomarkers (microRNA [miRNA] or messenger RNA [mRNA]) for identification of lymph node metastasis (LNM) in patients with invasive submucosal colorectal cancers (T1 CRC). In this study, we translated our tissue-based biomarkers into a blood-based liquid biopsy assay for noninvasive detection of LNM in patients with high-risk T1 CRC.
Methods: We analyzed 330 specimens from patients with high-risk T1 CRC, which included 188 serum samples from 2 clinical cohorts-a training cohort (N = 46) and a validation cohort (N = 142)-and matched formalin-fixed paraffin-embedded samples (N = 142). We performed quantitative reverse-transcription polymerase chain reaction, followed by logistic regression analysis, to develop an integrated transcriptomic panel and establish a risk-stratification model combined with clinical risk factors.
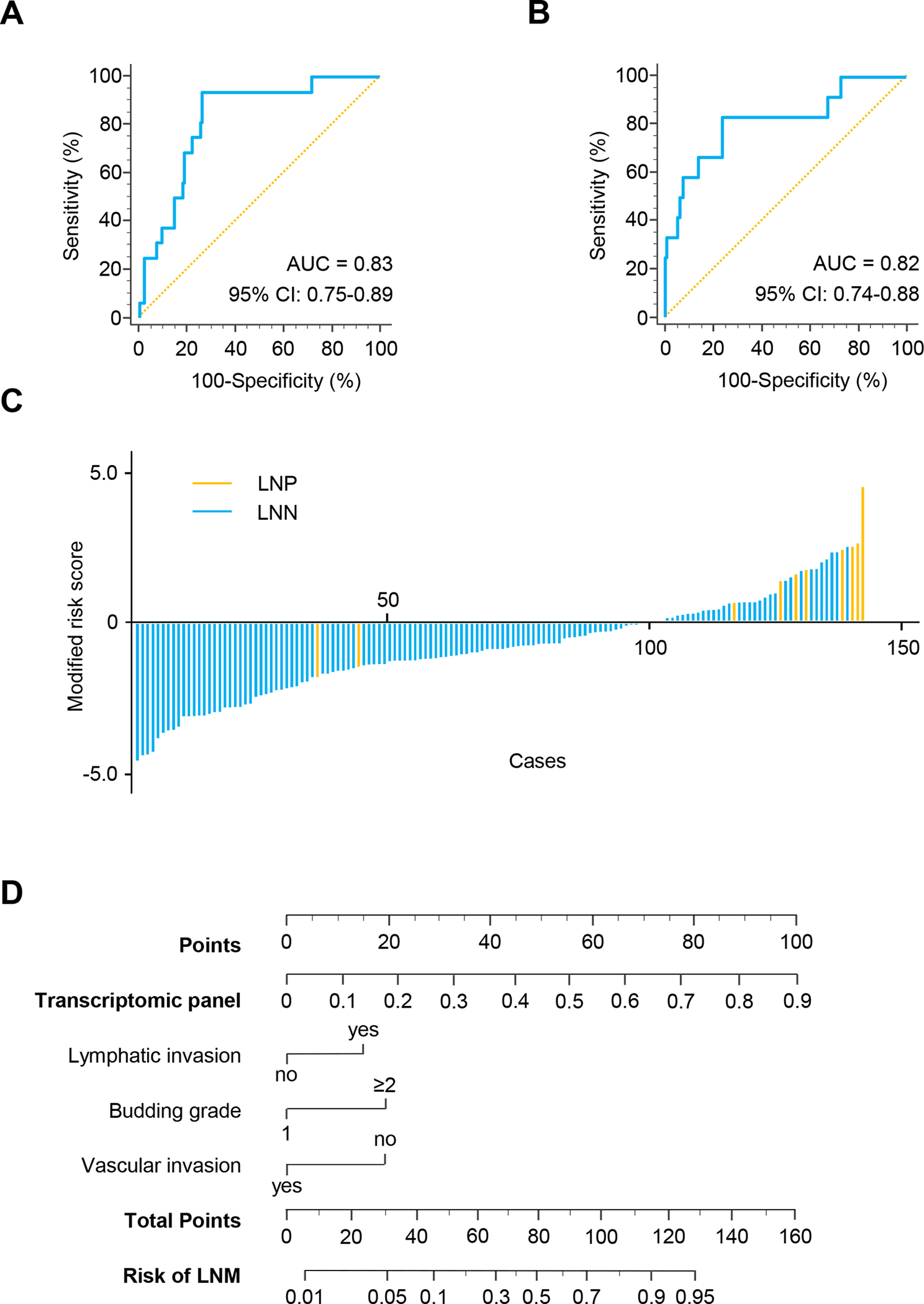
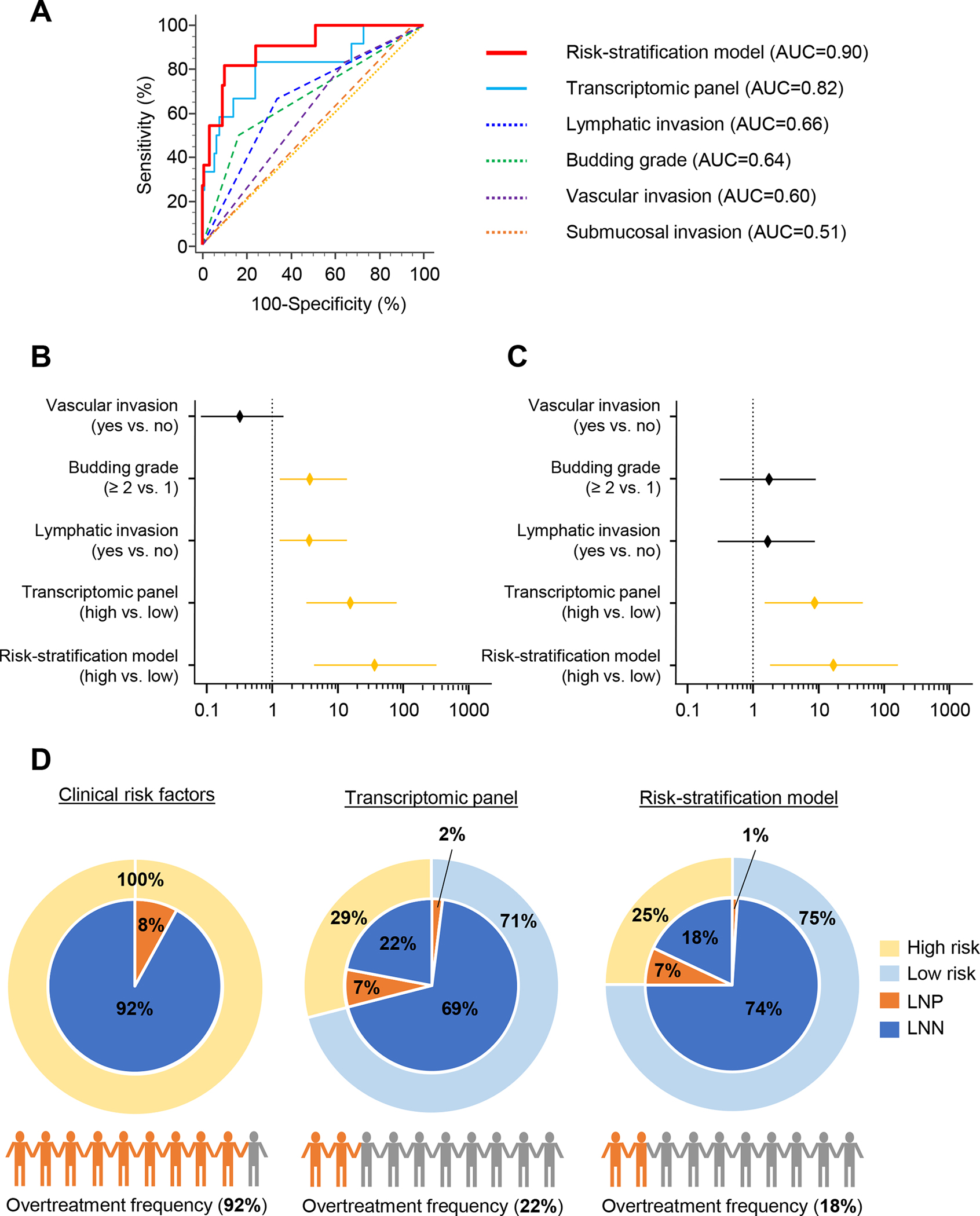
Results: We used comprehensive expression profiling of a training cohort of LNM-positive and LMN-negative serum specimens to identify an optimized transcriptomic panel of 4 miRNAs (miR-181b, miR-193b, miR-195, and miR-411) and 5 mRNAs (AMT, forkhead box A1 [FOXA1], polymeric immunoglobulin receptor [PIGR], matrix metalloproteinase 1 [MMP1], and matrix metalloproteinase 9 [MMP9]), which robustly identified patients with LNM (area under the curve [AUC], 0.86; 95% confidence interval [CI], 0.72-0.94). We validated panel performance in an independent validation cohort (AUC, 0.82; 95% CI, 0.74-0.88). Our risk-stratification model was more accurate than the panel and an independent predictor for identification of LNM (AUC, 0.90; univariate: odds ratio [OR], 37.17; 95% CI, 4.48-308.35; P < .001; multivariate: OR, 17.28; 95% CI, 1.82-164.07; P = .013). The model limited potential overtreatment to only 18% of all patients, which is dramatically superior to pathologic features that are currently used (92%).
Conclusions: A novel risk-stratification model for noninvasive identification of T1 CRC has the potential to avoid unnecessary operations for patients classified as high-risk by conventional risk-classification criteria.
Keywords: Detection Biomarker; Noninvasive Assay; Risk-Stratification Model; Transcriptomic Panel.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: None of the authors has any potential conflicts to disclose.
Figures
Comment in
-
Blood-Based Liquid Biopsies: A Noninvasive and Cost-Effective Tool for Improved Risk Assessment and Identification of Lymph Node Metastasis in Patients With Submucosal T1 Colorectal Cancer.Gastroenterology. 2021 Jul;161(1):29-31. doi: 10.1053/j.gastro.2021.04.038. Epub 2021 Apr 22. Gastroenterology. 2021. PMID: 33895167 No abstract available.
-
Noninvasive Identification of Lymph Node Metastasis in T1 Colorectal Cancer by Transcriptomic Panel Based on Liquid Biopsy Assay: Additional Analytical Strategies Are Needed.Gastroenterology. 2022 Jan;162(1):347-348. doi: 10.1053/j.gastro.2021.06.075. Epub 2021 Jul 2. Gastroenterology. 2022. PMID: 34224742 No abstract available.
References
-
- Stamos MJ, Murrell Z. Management of early rectal T1 and T2 cancers. Clin Cancer Res 2007;13:6885s–9s. - PubMed
-
- Iida S, Hasegawa H, Okabayashi K, et al. Risk factors for postoperative recurrence in patients with pathologically T1 colorectal cancer. World J Surg 2012;36:424–30. - PubMed
-
- Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc 2015;27:417–434. - PubMed
-
- Shimura T, Ebi M, Yamada T, et al. Magnifying chromoendoscopy and endoscopic ultrasonography measure invasion depth of early stage colorectal cancer with equal accuracy on the basis of a prospective trial. Clin Gastroenterol Hepatol 2014;12:662–8 e1–2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
