

Anthropometry at discharge and risk of relapse in children treated for severe acute malnutrition: a prospective cohort study in rural Nepal
- PMID: 33820545
- PMCID: PMC8021301
- DOI: 10.1186/s12937-021-00684-7
Anthropometry at discharge and risk of relapse in children treated for severe acute malnutrition: a prospective cohort study in rural Nepal
Abstract
Background: There is a dearth of evidence on what should be the optimal criteria for discharging children from severe acute malnutrition (SAM) treatment. Programs discharging children while they are still presenting varying levels of weight-for-height (WHZ) or mid-upper-arm circumference (MUAC) deficits, such as those implemented under the current national protocol in Nepal, are opportunities to fill this evidence gap.
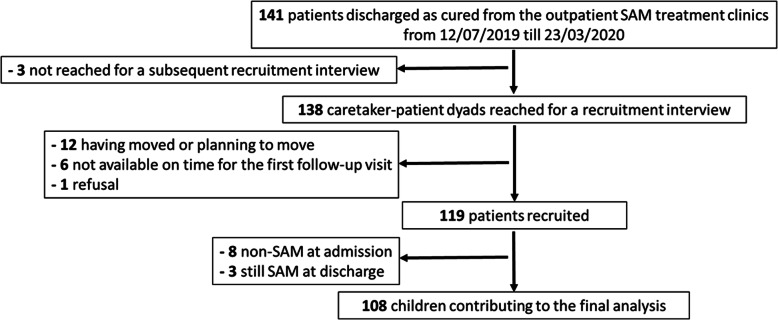
Methods: We followed a cohort of children discharged as cured from SAM treatment in Parasi district, Nepal. Relapse as SAM, defined as the occurrence of WHZ<-3 or MUAC < 115 mm or nutritional edema, was investigated through repeated home visits, during six months after discharge. We assessed the contribution of remaining anthropometric deficits at discharge to relapse risk through Cox regressions.
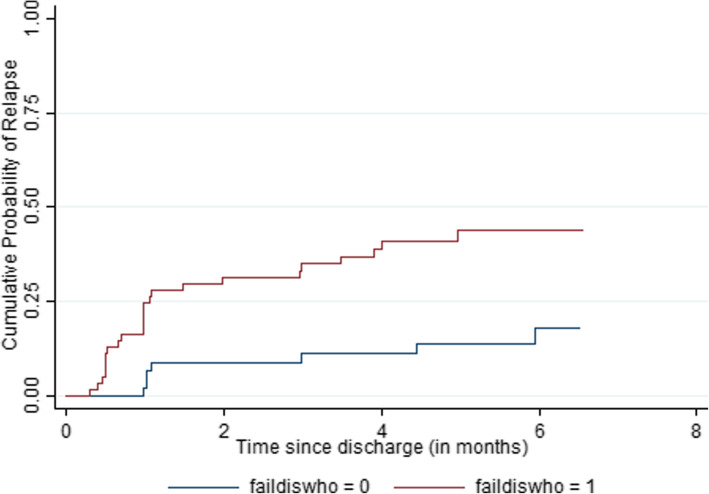
Results: Relapse as SAM during follow-up was observed in 33 % of the cohort (35/108). Being discharged before reaching the internationally recommended criteria was overall associated with a large increase in the risk of relapse (HR = 3.3; p = 0.006). Among all anthropometric indicators at discharge, WHZ<-2 led to a three-fold increase in relapse risk (HR = 3.2; p = 0.003), while MUAC < 125 mm significantly raised it only in the older children. WHZ<-2 at discharge came up as the only significant predictor of relapse in multivariate analysis (HR = 2.8, p = 0.01), even among children with a MUAC ≥ 125 mm. Of note, more than 80 % of the events of relapse as SAM would have been missed if WHZ had not been monitored and used in the definition of relapse.
Conclusions: Our results suggest that the priority for SAM management programs should be to ensure that children reach a high level of WHZ at discharge, at least above or equal to the WHO recommended cut-off. The validity of using a single MUAC cut-off such as 125 mm as a suitable discharge criterion for all age groups is questioned. Further follow-up studies providing a complete assessment of nutritional status at discharge and not based on a restricted MUAC-only definition of relapse as SAM would be urgently needed to set evidence-based discharge criteria. These studies are also required to assess programs currently discounting or omitting WHZ for identification and management of SAM.
Keywords: Discharge; MUAC; Relapse; Severe acute malnutrition; WHZ.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- UNICEF/WHO/The World Bank Group joint child. malnutrition estimates: levels and trends in child malnutrition: key findings of the 2020 edition. . Accessed 27 Oct 2020.
-
- World Health Organization, UNICEF. WHO child growth standards and the identification of severe acute malnutrition in infants and children: a joint statement by the World Health Organization and the United Nations Children’s Fund. 2009. . Accessed 27 Oct 2020. - PubMed
-
- World Health Organization. WHO. Guideline: Updates on the management of severe acute malnutrition in infants and children; 2013. Geneva: World Health Organization. 2013. . Accessed 6 Nov 2020. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
