

Actual survival after resection of primary colorectal cancer: results from a prospective multicenter study
- PMID: 33820567
- PMCID: PMC8022415
- DOI: 10.1186/s12957-021-02207-4
Actual survival after resection of primary colorectal cancer: results from a prospective multicenter study
Erratum in
-
Correction to: Actual survival after resection of primary colorectal cancer: results from a prospective multicenter study.World J Surg Oncol. 2021 May 26;19(1):159. doi: 10.1186/s12957-021-02252-z. World J Surg Oncol. 2021. PMID: 34039352 Free PMC article. No abstract available.
Abstract
Background: Colorectal cancer is the third most common type of cancer in the world. We characterize a cohort of patients who survived up to 5 years without recurrence and identify factors predicting the probability of cure.
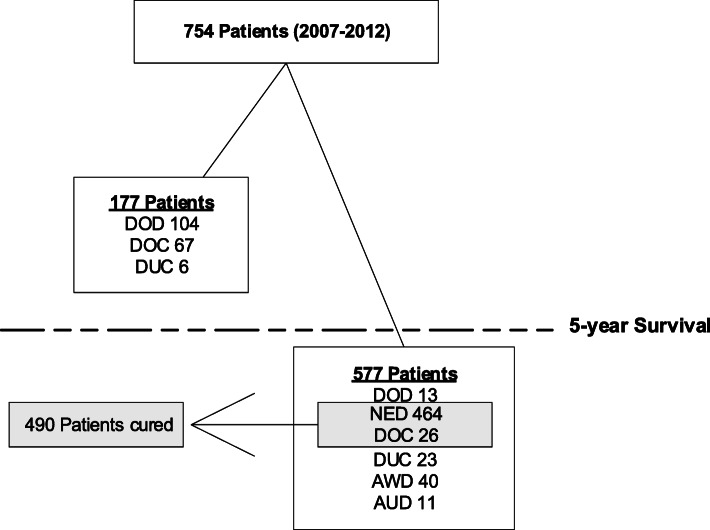
Methods: We analyzed data of patients who underwent curative intent surgery for stage I-III CRC between 2007 and 2012 and who had had been included in a large multicenter study in the Netherlands. Cure was defined as 5-year survival without recurrence. Survival data were retrieved from a national registry.
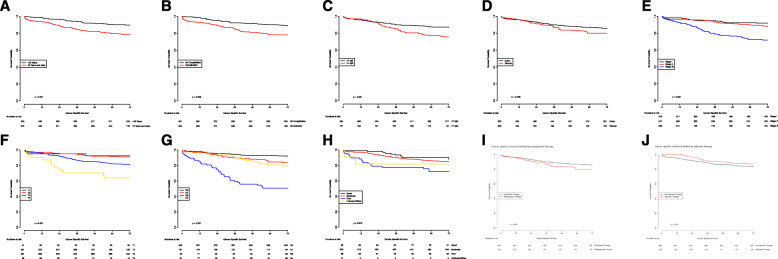
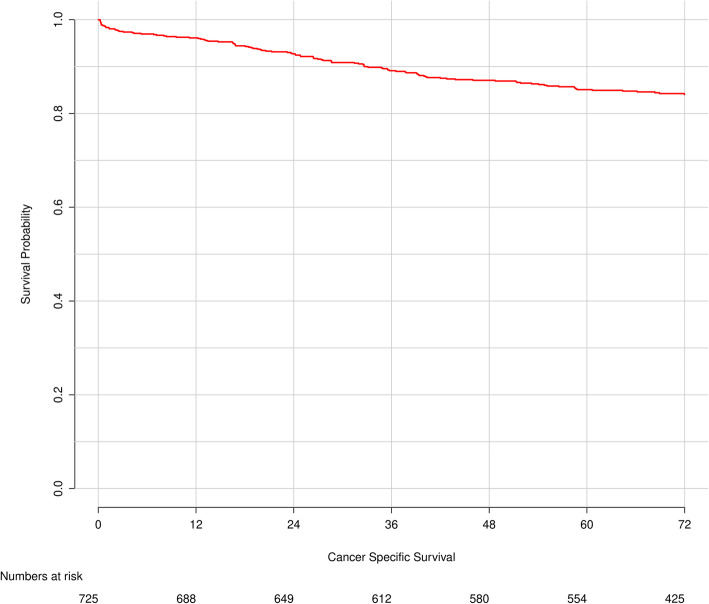
Results: Analysis of data of 754 patients revealed a cure rate of 65% (n = 490). Patients with stage I disease and T1- and N0-tumor had the highest probability of cure (94%, 95% and 90%, respectively). Those with a T4-tumor or N2-tumor had the lowest probability of cure (62% and 50%, respectively). A peak in the mortality rate for older patients early in follow-up suggests early excess mortality as an explanation. A similar trend was observed for stage III disease, poor tumor grade, postoperative complications, sarcopenia, and R1 resections. Patients with stage III disease, poor tumor grade, postoperative complications, sarcopenia, and R1 resections show a similar trend for decrease in CSS deaths over time.
Conclusion: In the studied cohort, the probability of cure for patients with stage I-III CRC ranged from 50 to 95%. Even though most patients will be cured from CRC with standard therapy, standard therapy is insufficient for those with poor prognostic factors, such as high T- and N-stage and poor differentiation grade.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- The Global Cancer Observatory (GCO). https://gco.iarc.fr/. Accessed Aug 2020.
-
- Dienstmann R, Mason MJ, Sinicrope FA, Phipps AI, Tejpar S, Nesbakken A, Danielsen SA, Sveen A, Buchanan DD, Clendenning M, Rosty C, Bot B, Alberts SR, Milburn Jessup J, Lothe RA, Delorenzi M, Newcomb PA, Sargent D, Guinney J. Prediction of overall survival in stage II and III colon cancer beyond TNM system: a retrospective, pooled biomarker study. Ann Oncol. 2017;28(5):1023–1031. doi: 10.1093/annonc/mdx052. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
