

Impact of Cardiovascular Diseases on COVID-19: A Systematic Review
- PMID: 33820904
- PMCID: PMC8035813
- DOI: 10.12659/MSM.930032
Impact of Cardiovascular Diseases on COVID-19: A Systematic Review
Abstract
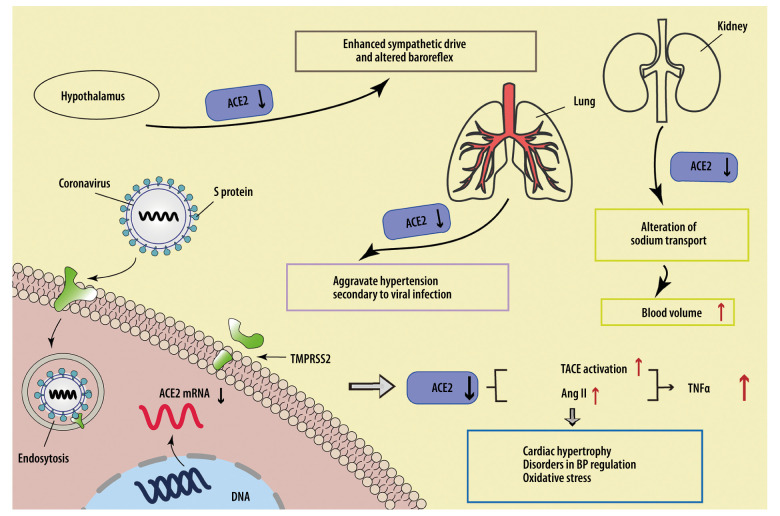
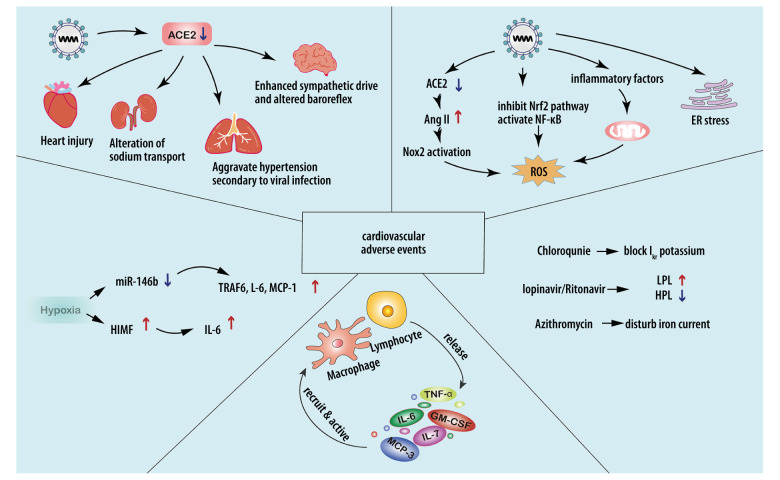
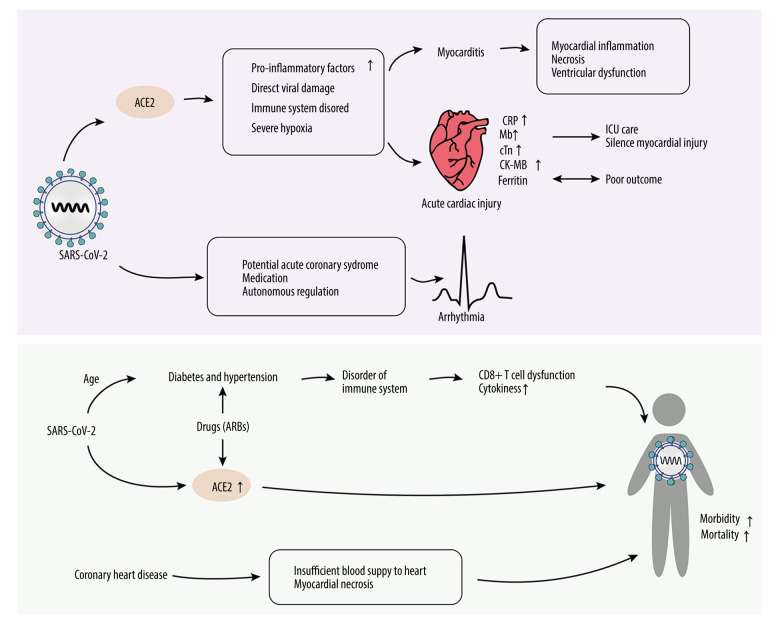
In December 2019, pneumonia of unknown cause broke out, and currently more than 150 countries around the world have been affected. Globally, as of 5: 46 pm CET, 6 November 2020, the World Health Organization (WHO) had reported 48 534 508 confirmed cases of COVID-19, including 1 231 017 deaths. The novel coronavirus disease (COVID-19) outbreak, caused by the SARS-CoV-2 virus, is the most important medical challenge in decades. Previous research mainly focused on the exploration of lung changes. However, with development of the disease and deepening research, more and more patients showed cardiovascular diseases, even in those without respiratory symptoms, and some researchers have found that underlying cardiovascular diseases increase the risk of infection. Although the related mechanism is not thoroughly studied, based on existing research, we speculate that the interaction between the virus and its receptor, inflammatory factors, various forms of the stress response, hypoxic environment, and drug administration could all induce the development of cardiac adverse events. Interventions to control these pathogenic factors may effectively reduce the occurrence of cardiovascular complications. This review summarizes the latest research on the relationship between COVID-19 and its associated cardiovascular complications, and we also explore possible mechanisms and treatments.
Conflict of interest statement
None.
Figures
Similar articles
-
Pathogenesis-directed therapy of 2019 novel coronavirus disease.J Med Virol. 2021 Mar;93(3):1320-1342. doi: 10.1002/jmv.26610. Epub 2020 Nov 10. J Med Virol. 2021. PMID: 33073355 Review.
-
Management of acute cardiovascular events in patients with COVID-19.Rev Cardiovasc Med. 2020 Dec 30;21(4):577-581. doi: 10.31083/j.rcm.2020.04.140. Rev Cardiovasc Med. 2020. PMID: 33388002 Review.
-
Pathogenesis and management of myocardial injury in coronavirus disease 2019.Eur J Heart Fail. 2020 Nov;22(11):1994-2006. doi: 10.1002/ejhf.1967. Epub 2020 Aug 22. Eur J Heart Fail. 2020. PMID: 32683753 Free PMC article. Review.
-
Pathophysiology and pharmacological management of pulmonary and cardiovascular features of COVID-19.J Mol Cell Cardiol. 2021 Apr;153:72-85. doi: 10.1016/j.yjmcc.2020.12.009. Epub 2020 Dec 26. J Mol Cell Cardiol. 2021. PMID: 33373644 Free PMC article.
-
Potential Effects of Coronaviruses on the Cardiovascular System: A Review.JAMA Cardiol. 2020 Jul 1;5(7):831-840. doi: 10.1001/jamacardio.2020.1286. JAMA Cardiol. 2020. PMID: 32219363 Review.
Cited by
-
Computational analysis of antimicrobial peptides targeting key receptors in infection-related cardiovascular diseases: molecular docking and dynamics insights.Sci Rep. 2025 Mar 14;15(1):8896. doi: 10.1038/s41598-025-93683-1. Sci Rep. 2025. PMID: 40087360 Free PMC article.
-
Cardiac Biomarkers and Their Role in Identifying Increased Risk of Cardiovascular Complications in COVID-19 Patients.Diagnostics (Basel). 2023 Jul 27;13(15):2508. doi: 10.3390/diagnostics13152508. Diagnostics (Basel). 2023. PMID: 37568870 Free PMC article. Review.
-
COVID-19 and Preexisting Comorbidities: Risks, Synergies, and Clinical Outcomes.Front Immunol. 2022 May 27;13:890517. doi: 10.3389/fimmu.2022.890517. eCollection 2022. Front Immunol. 2022. PMID: 35711466 Free PMC article. Review.
-
COVID-19-induced cardiovascular damage differs from other prevalent viruses.Cardiol Plus. 2021 Oct 1;6(4):231-245. doi: 10.4103/2470-7511.334401. Epub 2021 Dec 30. Cardiol Plus. 2021. PMID: 35368975 Free PMC article. Review.
-
Emerging Role of Platelet-Endothelium Interactions in the Pathogenesis of Severe SARS-CoV-2 Infection-Associated Myocardial Injury.Front Immunol. 2022 Feb 4;13:776861. doi: 10.3389/fimmu.2022.776861. eCollection 2022. Front Immunol. 2022. PMID: 35185878 Free PMC article. Review.
References
-
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. [cited 2020, 8/31]. https://covid19.who.int/
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
