

1-13C-propionate breath testing as a surrogate endpoint to assess efficacy of liver-directed therapies in methylmalonic acidemia (MMA)
- PMID: 33820958
- PMCID: PMC8354855
- DOI: 10.1038/s41436-021-01143-8
1-13C-propionate breath testing as a surrogate endpoint to assess efficacy of liver-directed therapies in methylmalonic acidemia (MMA)
Erratum in
-
Correction to: 1-13C-propionate breath testing as a surrogate endpoint to assess efficacy of liver-directed therapies in methylmalonic acidemia (MMA).Genet Med. 2021 Nov;23(11):2233. doi: 10.1038/s41436-021-01188-9. Genet Med. 2021. PMID: 33972722 Free PMC article. No abstract available.
Abstract
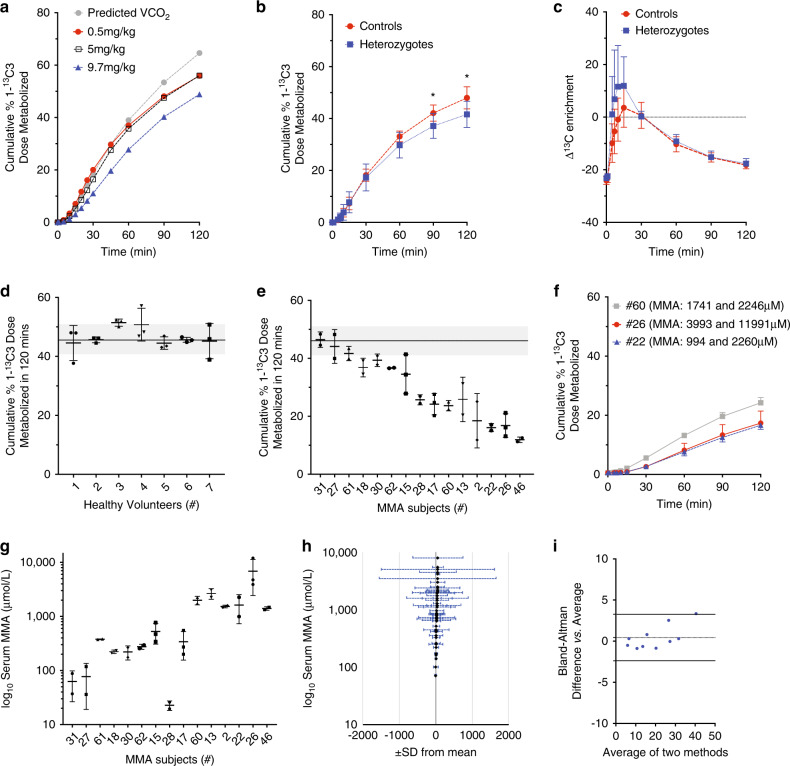
Purpose: To develop a safe and noninvasive in vivo assay of hepatic propionate oxidative capacity.
Methods: A modified 1-13C-propionate breath test was administered to 57 methylmalonic acidemia (MMA) subjects, including 19 transplant recipients, and 16 healthy volunteers. Isotopomer enrichment (13CO2/12CO2) was measured in exhaled breath after an enteral bolus of sodium-1-13C-propionate, and normalized for CO2 production. 1-13C-propionate oxidation was then correlated with clinical, laboratory, and imaging parameters collected via a dedicated natural history protocol.
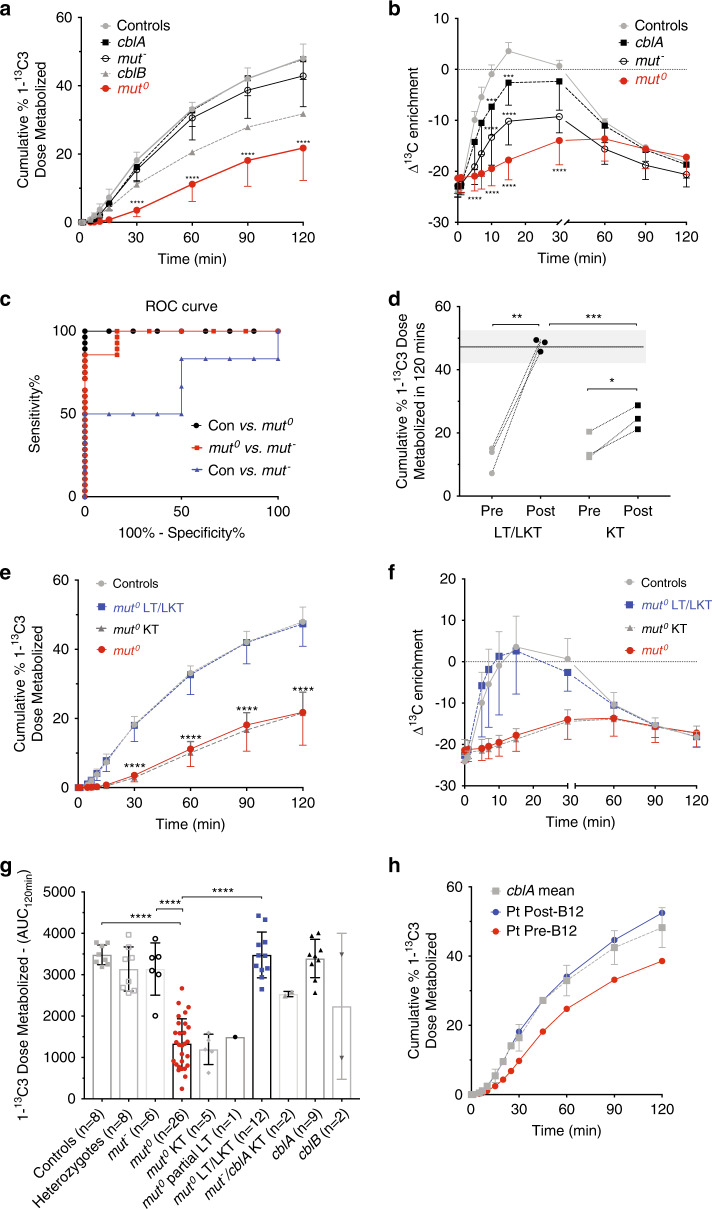
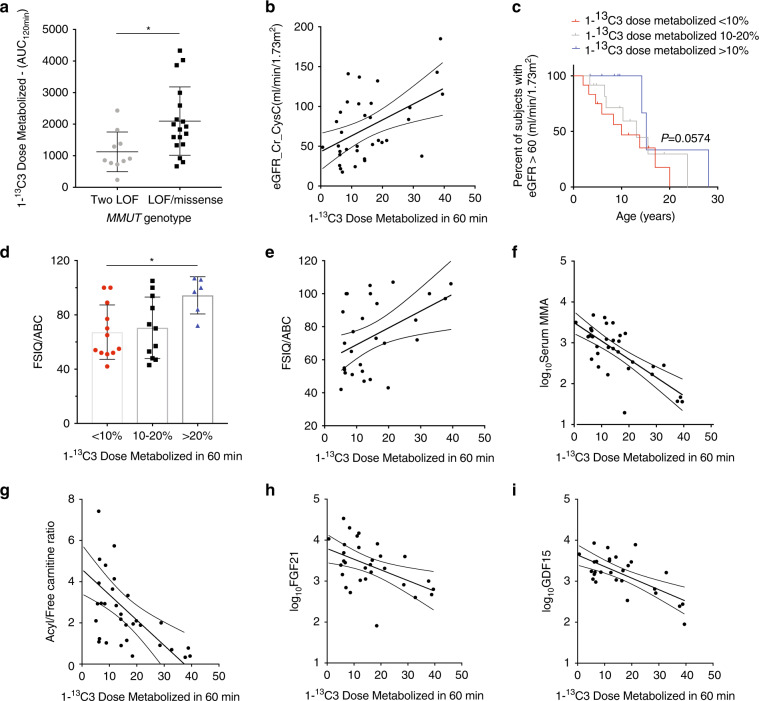
Results: Lower propionate oxidation was observed in patients with the severe mut0 and cblB subtypes of MMA, but was near normal in those with the cblA and mut- forms of the disorder. Liver transplant recipients demonstrated complete restoration of 1-13C-propionate oxidation to control levels. 1-13C-propionate oxidation correlated with cognitive test result, growth indices, bone mineral density, renal function, and serum biomarkers. Test repeatability was robust in controls and in MMA subjects (mean coefficient of variation 6.9% and 12.8%, respectively), despite widely variable serum methylmalonic acid concentrations in the patients.
Conclusion: Propionate oxidative capacity, as measured with 1-13C-propionate breath testing, predicts disease severity and clinical outcomes, and could be used to assess the therapeutic effects of liver-targeted genomic therapies for MMA and related disorders of propionate metabolism.
Trial registration: This clinical study is registered in www.clinicaltrials.gov with the ID: NCT00078078. Study URL: http://clinicaltrials.gov/ct2/show/NCT00078078.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
I.M and C.P.V. are inventors on patents related to isotopic biomarkers in organic acidemias filed by the NIH on their behalf. The other authors declare no competing interests.
Figures
References
-
- Manoli, I., Sloan, J. L. & Venditti, C. P. in GeneReviews (eds Pagon, R. A. et al.) Isolated methylmalonic acidemia (University of Washington, Seattle, 2016).
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
