

Alterations in T and B cell function persist in convalescent COVID-19 patients
- PMID: 33821250
- PMCID: PMC8011689
- DOI: 10.1016/j.medj.2021.03.013
Alterations in T and B cell function persist in convalescent COVID-19 patients
Abstract
Background: Emerging studies indicate that some coronavirus disease 2019 (COVID-19) patients suffer from persistent symptoms, including breathlessness and chronic fatigue; however, the long-term immune response in these patients presently remains ill-defined.
Methods: Here, we describe the phenotypic and functional characteristics of B and T cells in hospitalized COVID-19 patients during acute disease and at 3-6 months of convalescence.
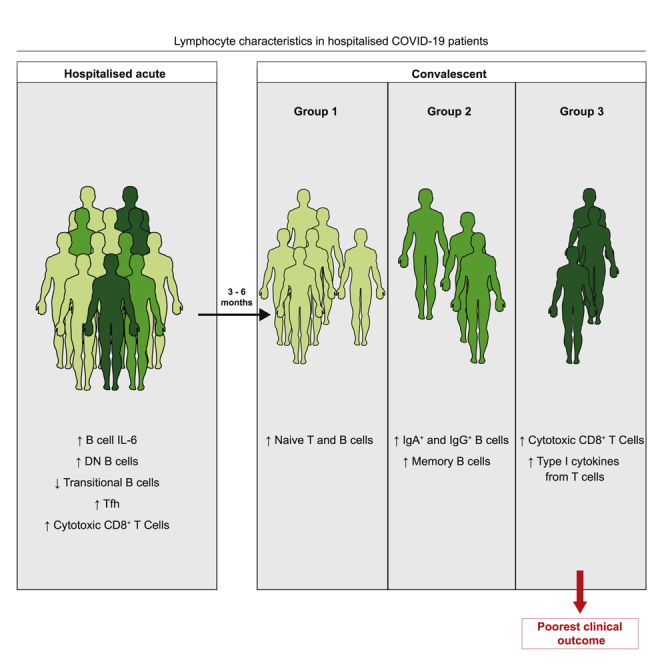
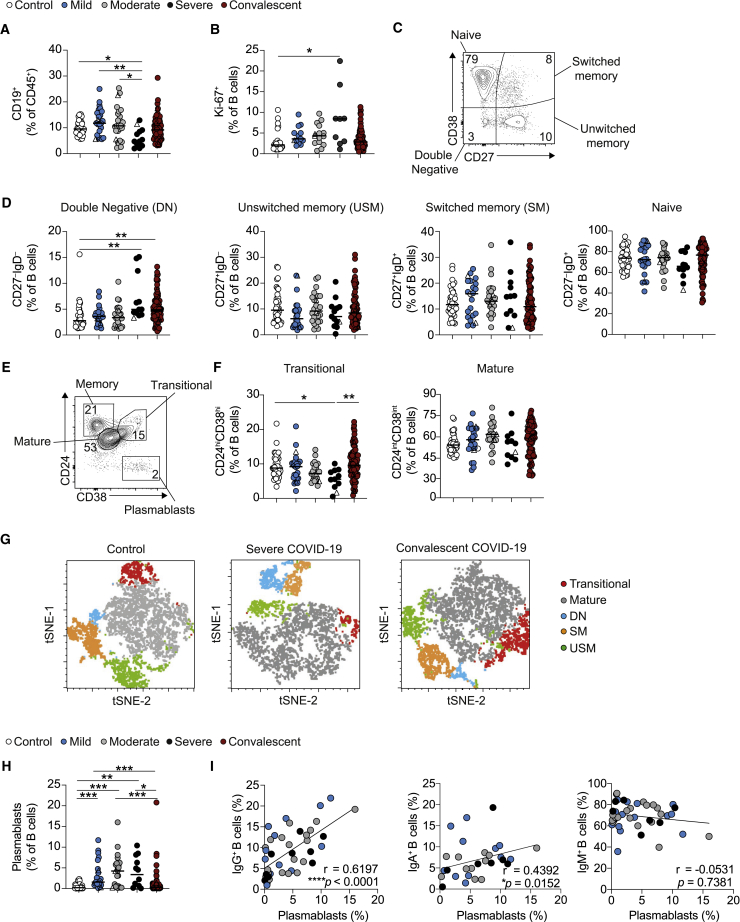
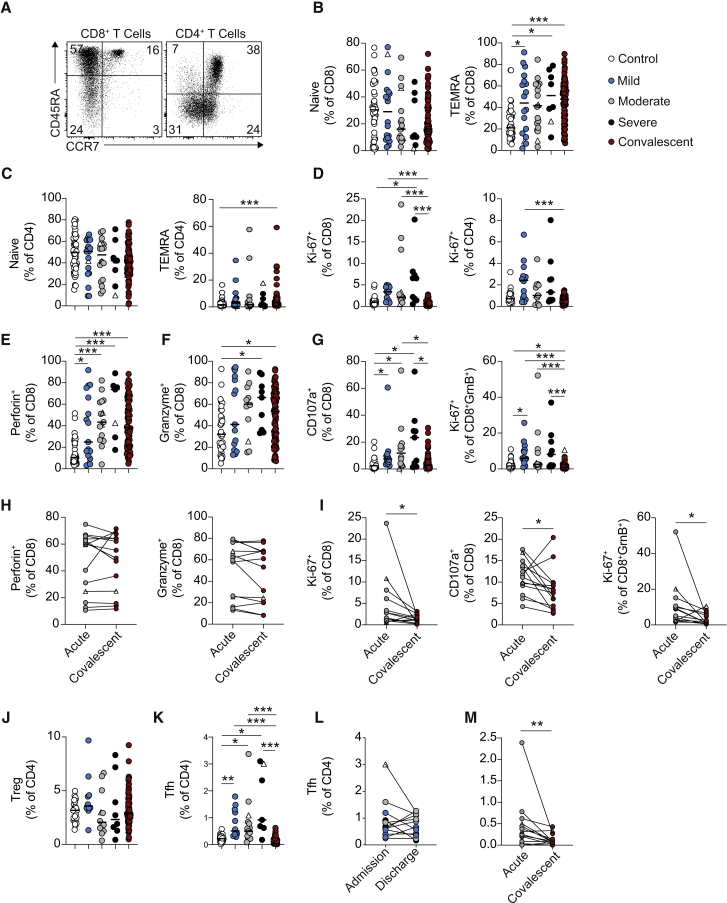
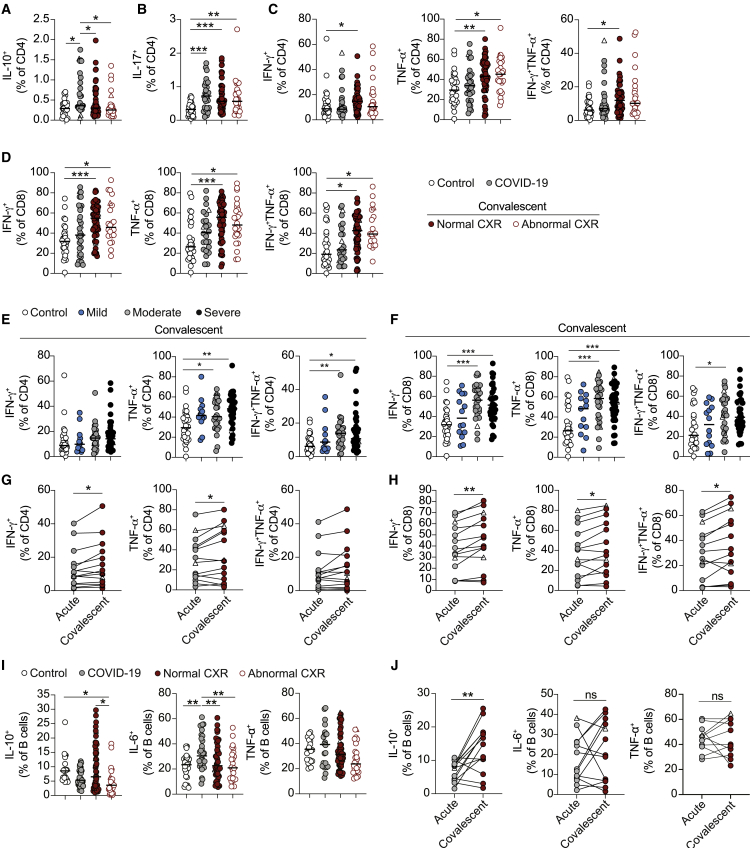
Findings: We report that the alterations in B cell subsets observed in acute COVID-19 patients were largely recovered in convalescent patients. In contrast, T cells from convalescent patients displayed continued alterations with persistence of a cytotoxic program evident in CD8+ T cells as well as elevated production of type 1 cytokines and interleukin-17 (IL-17). Interestingly, B cells from patients with acute COVID-19 displayed an IL-6/IL-10 cytokine imbalance in response to Toll-like receptor activation, skewed toward a pro-inflammatory phenotype. Whereas the frequency of IL-6+ B cells was restored in convalescent patients irrespective of clinical outcome, the recovery of IL-10+ B cells was associated with the resolution of lung pathology.
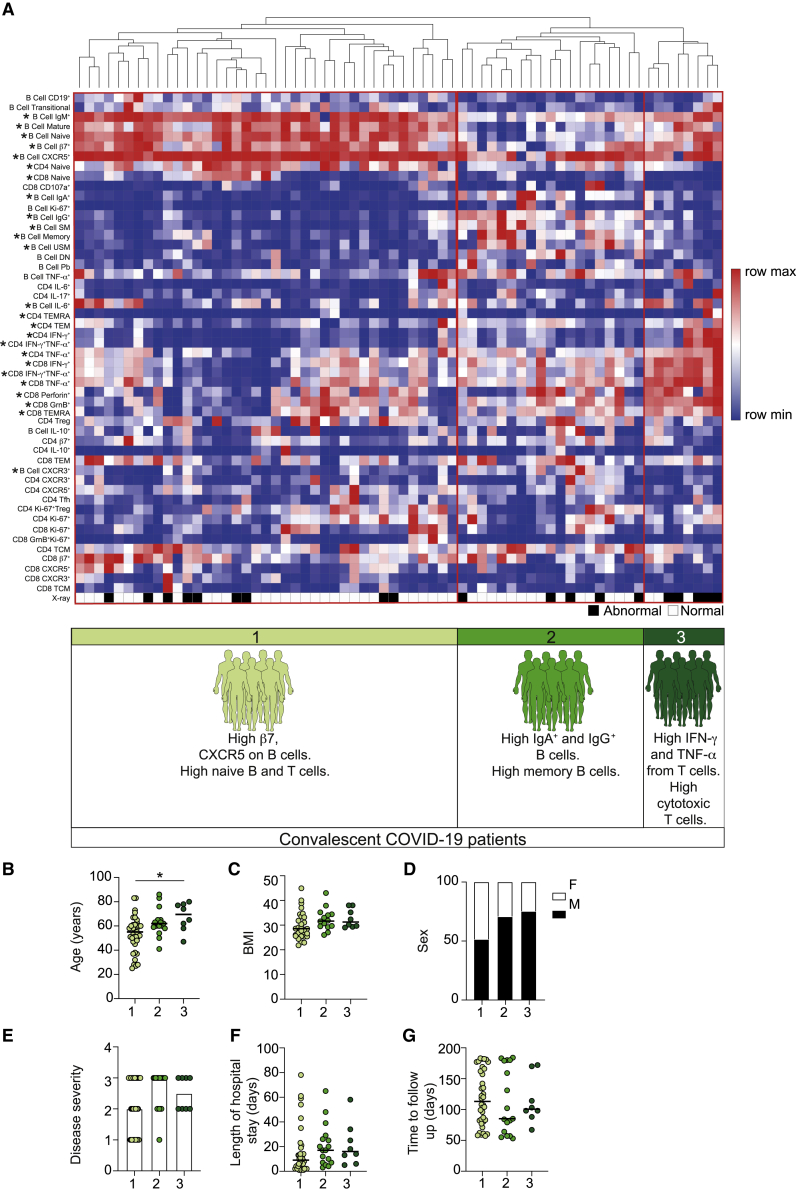
Conclusions: Our data detail lymphocyte alterations in previously hospitalized COVID-19 patients up to 6 months following hospital discharge and identify 3 subgroups of convalescent patients based on distinct lymphocyte phenotypes, with 1 subgroup associated with poorer clinical outcome. We propose that alterations in B and T cell function following hospitalization with COVID-19 could affect longer-term immunity and contribute to some persistent symptoms observed in convalescent COVID-19 patients.
Funding: Provided by UKRI, Lister Institute of Preventative Medicine, the Wellcome Trust, The Kennedy Trust for Rheumatology Research, and 3M Global Giving.
Keywords: B cells; COVID-19; T cells; convalescent patients; long COVID; viral Infection.
© 2021 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- 21927/VAC_/Versus Arthritis/United Kingdom
- MR/V028448/1/MRC_/Medical Research Council/United Kingdom
- 202865/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- BB/M025977/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- BB/S01103X/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
