

MRI-based diagnosis and treatment of pediatric brain tumors: is tissue sample always needed?
- PMID: 33821340
- PMCID: PMC8084800
- DOI: 10.1007/s00381-021-05148-1
MRI-based diagnosis and treatment of pediatric brain tumors: is tissue sample always needed?
Abstract
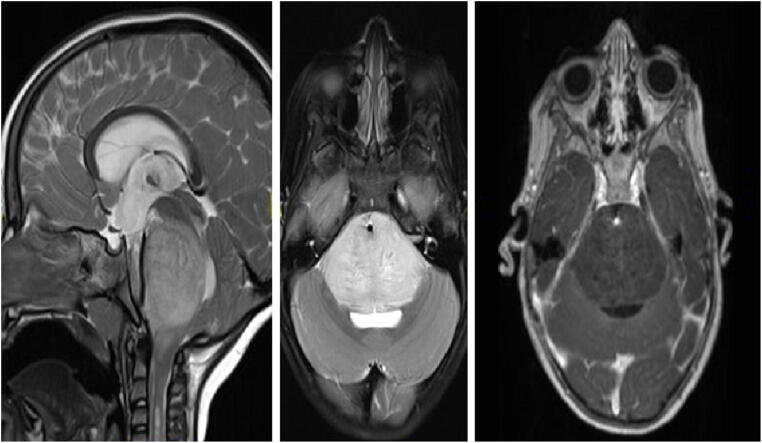
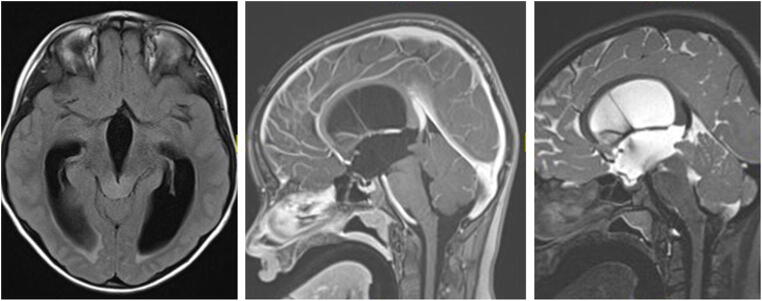
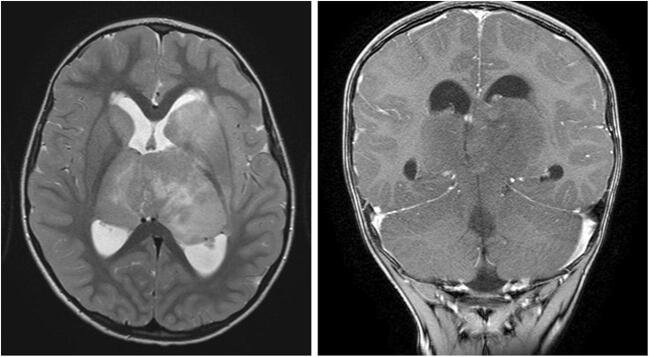
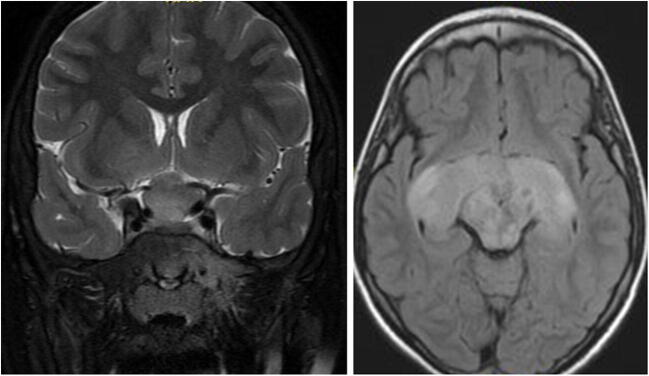
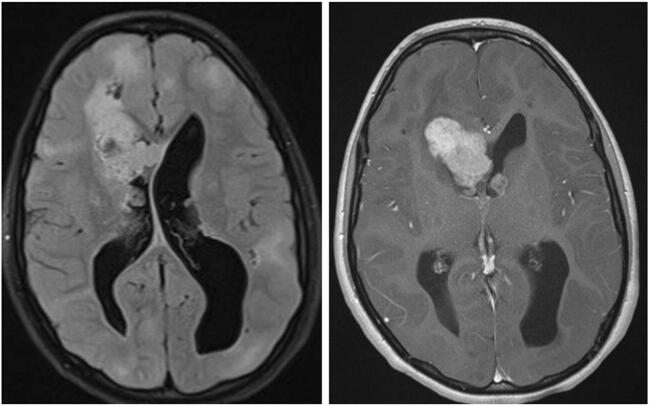
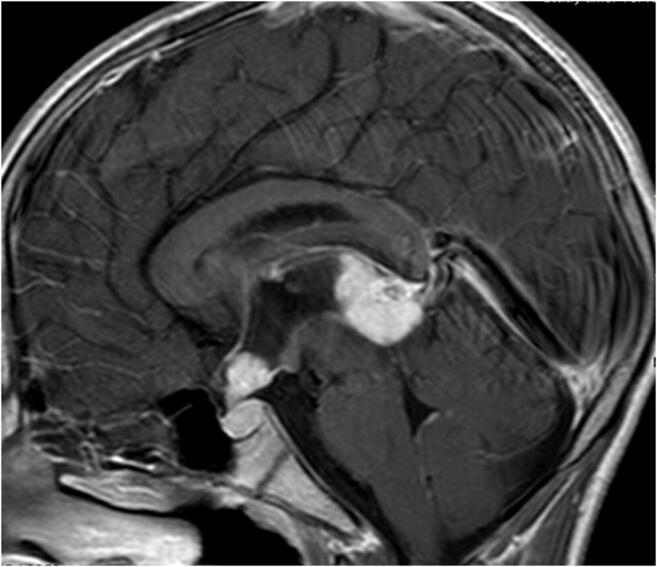
Traditional management of newly diagnosed pediatric brain tumors (PBTs) consists of cranial imaging, typically magnetic resonance imaging (MRI), and is frequently followed by tissue diagnosis, through either surgical biopsy or tumor resection. Therapy regimes are typically dependent on histological diagnosis. To date, many treatment regimens are based on molecular biology. The scope of this article is to discuss the role of diagnosis and further treatment of PBTs based solely on MRI features, in light of the latest treatment protocols. Typical MRI findings and indications for surgical biopsy of these lesions are described.
Keywords: Image-based diagnosis; Magnetic resonance imaging; Pediatric brain tumors; Pediatric neuroradiology; Pediatric neurosurgery; Surgical biopsy.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
