

Left Ventricular Dysfunction in Arrhythmogenic Cardiomyopathy: Association With Exercise Exposure, Genetic Basis, and Prognosis
- PMID: 33821670
- PMCID: PMC8174162
- DOI: 10.1161/JAHA.120.018680
Left Ventricular Dysfunction in Arrhythmogenic Cardiomyopathy: Association With Exercise Exposure, Genetic Basis, and Prognosis
Abstract
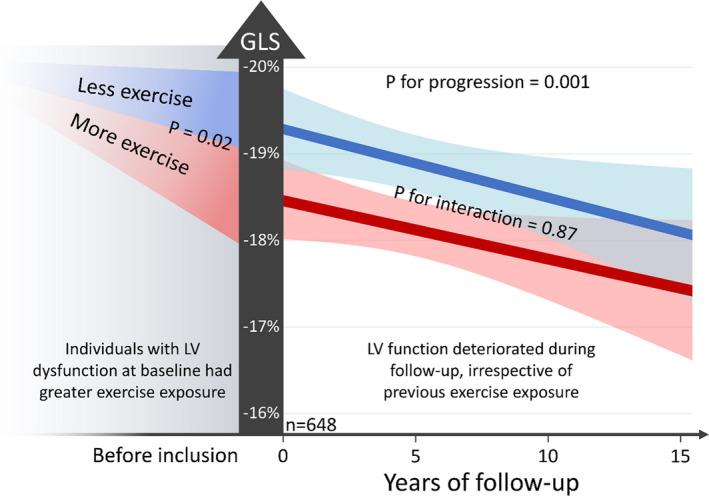
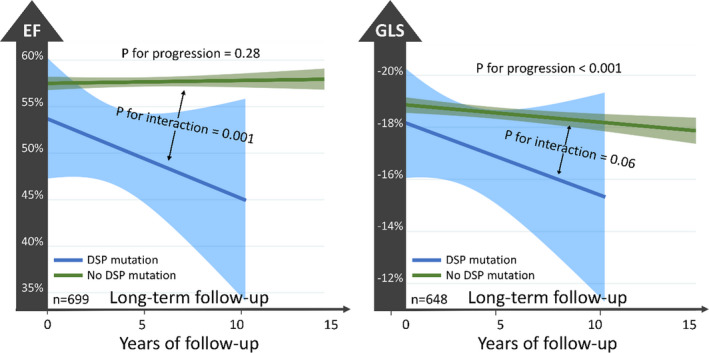
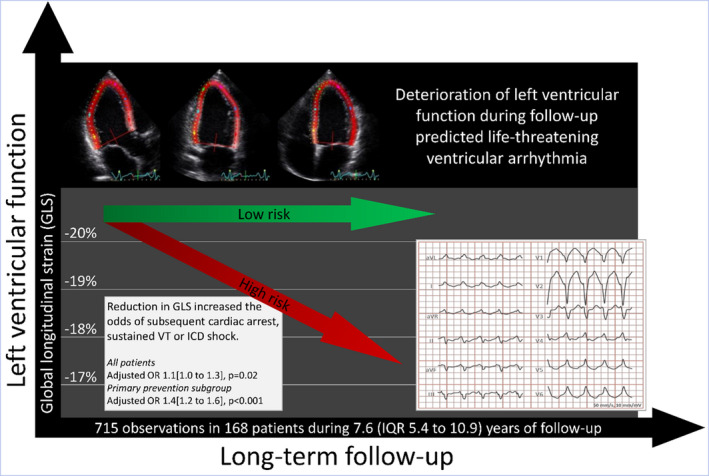
Background Arrhythmogenic cardiomyopathy (AC) is characterized by biventricular dysfunction, exercise intolerance, and high risk of ventricular tachyarrhythmias and sudden death. Predisposing factors for left ventricular (LV) disease manifestation and its prognostic implication in AC are poorly described. We aimed to assess the associations of exercise exposure and genotype with LV dysfunction in AC, and to explore the impact of LV disease progression on adverse arrhythmic outcome. Methods and Results We included 168 patients with AC (50% probands, 45% women, 40±16 years old) with 715 echocardiographic exams (4.1±1.7 exams/patient, follow-up 7.6 [interquartile range (IQR), 5.4-10.9] years) and complete exercise and genetic data in a longitudinal study. LV function by global longitudinal strain was -18.8% [IQR, -19.2% to -18.3%] at presentation and was worse in patients with greater exercise exposure (global longitudinal strain worsening, 0.09% [IQR, 0.01%-0.17%] per 5 MET-hours/week, P=0.02). LV function by global longitudinal strain worsened, with 0.08% [IQR, 0.05%-0.12%] per year; (P<0.001), and progression was most evident in patients with desmoplakin genotype (P for interaction <0.001). Deterioration of LV function predicted incident ventricular tachyarrhythmia (aborted cardiac arrest, sustained ventricular tachycardia, or implantable cardioverter defibrillator shock) (adjusted odds ratio, 1.1 [IQR, 1.0-1.3] per 1% worsening by global longitudinal strain; P=0.02, adjusted for time and previous arrhythmic events). Conclusions Greater exercise exposure was associated with worse LV function at first visit of patients with AC but did not significantly affect the rate of LV progression during follow-up. Progression of LV dysfunction was most pronounced in patients with desmoplakin genotypes. Deterioration of LV function during follow-up predicted subsequent ventricular tachyarrhythmia and should be considered in risk stratification.
Keywords: arrhythmogenic cardiomyopathy; arrhythmogenic right ventricular cardiomyopathy; left ventricular dysfunction; ventricular arrhythmia.
Conflict of interest statement
None.
Figures
References
-
- Lie ØH, Rootwelt‐Norberg C, Dejgaard LA, Leren IS, Stokke MK, Edvardsen T, Haugaa KH. Prediction of life‐threatening ventricular arrhythmia in patients with arrhythmogenic cardiomyopathy: a primary prevention cohort study. J Am Coll Cardiol Img. 2018;11:1377–1386. DOI: 10.1016/j.jcmg.2018.05.017. - DOI - PubMed
-
- Mast TP, Teske AJ, vd Heijden JF, Groeneweg JA, Te Riele ASJM, Velthuis BK, Hauer RNW, Doevendans PA, Cramer MJ. Left ventricular involvement in arrhythmogenic right ventricular dysplasia/cardiomyopathy assessed by echocardiography predicts adverse clinical outcome. J Am Soc Echocardiogr. 2015;28:1103–1113. DOI: 10.1016/j.echo.2015.04.015. - DOI - PubMed
-
- Ruwald AC, Marcus F, Estes NA 3rd, Link M, McNitt S, Polonsky B, Calkins H, Towbin JA, Moss AJ, Zareba W. Association of competitive and recreational sport participation with cardiac events in patients with arrhythmogenic right ventricular cardiomyopathy: results from the North American multidisciplinary study of arrhythmogenic right ventricular cardiomyopathy. Eur Heart J. 2015;36:1735–1743. DOI: 10.1093/eurheartj/ehv110. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
