

Cognitive impairment and altered cerebral glucose metabolism in the subacute stage of COVID-19
- PMID: 33822001
- PMCID: PMC8083602
- DOI: 10.1093/brain/awab009
Cognitive impairment and altered cerebral glucose metabolism in the subacute stage of COVID-19
Abstract
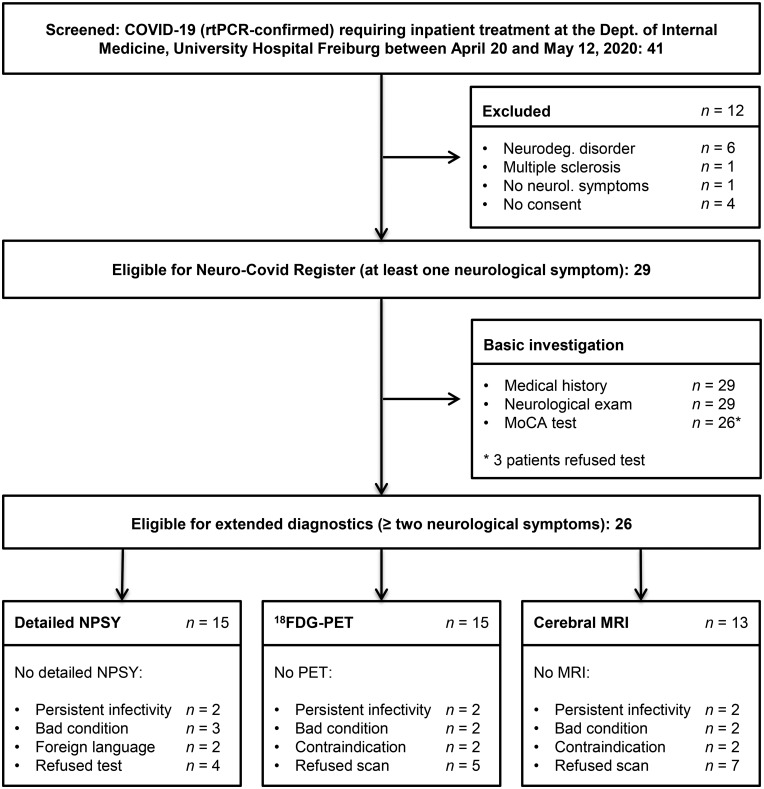
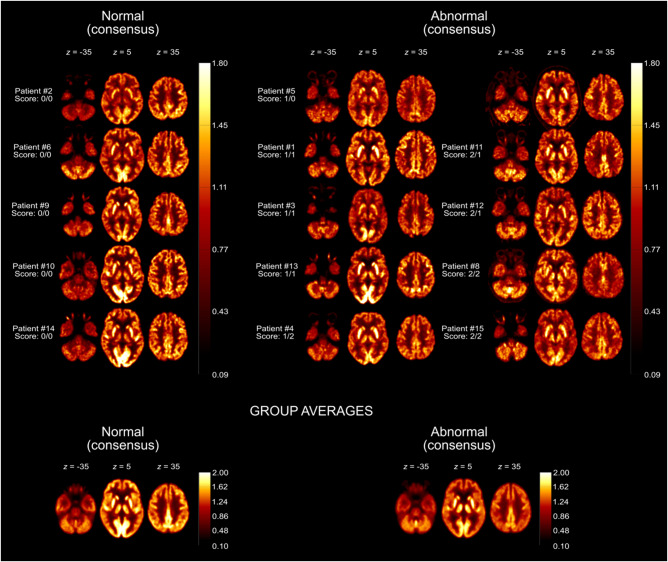
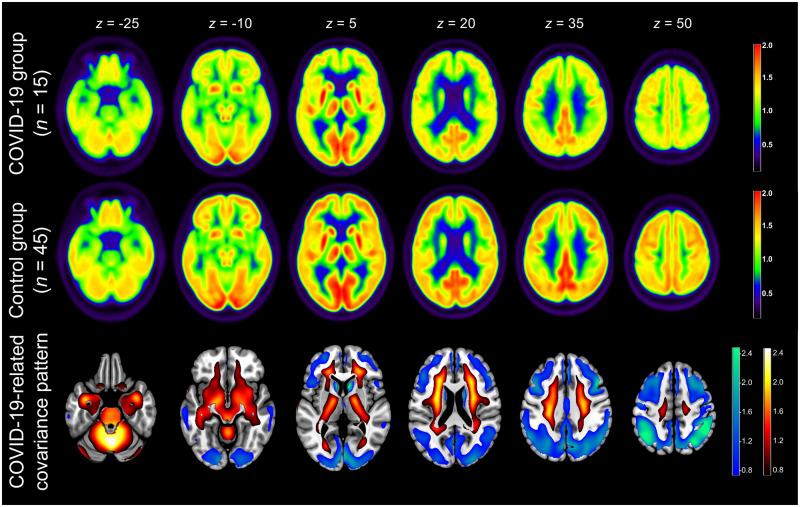
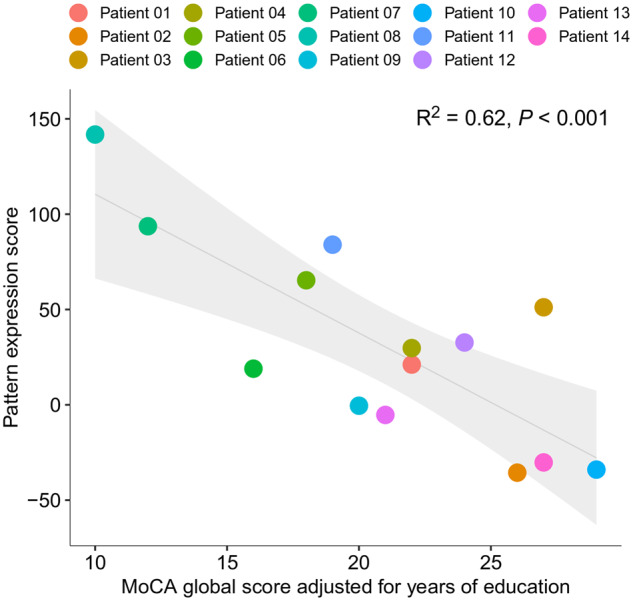
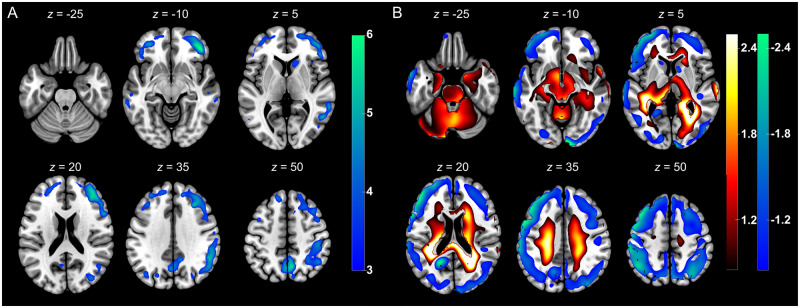
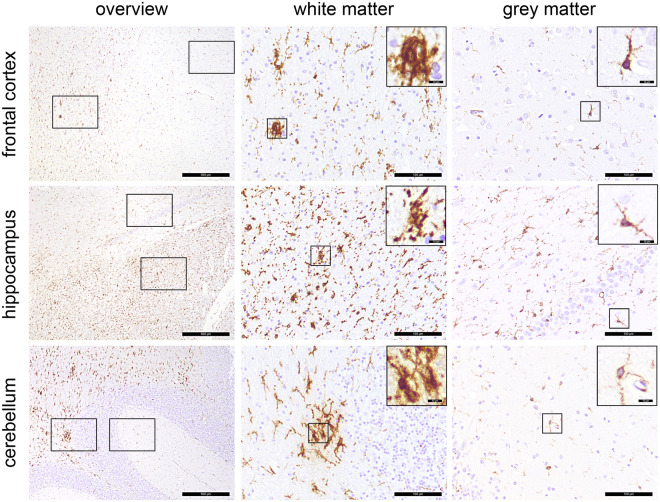
During the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, neurological symptoms increasingly moved into the focus of interest. In this prospective cohort study, we assessed neurological and cognitive symptoms in hospitalized coronavirus disease-19 (COVID-19) patients and aimed to determine their neuronal correlates. Patients with reverse transcription-PCR-confirmed COVID-19 infection who required inpatient treatment primarily because of non-neurological complications were screened between 20 April 2020 and 12 May 2020. Patients (age > 18 years) were included in our cohort when presenting with at least one new neurological symptom (defined as impaired gustation and/or olfaction, performance < 26 points on a Montreal Cognitive Assessment and/or pathological findings on clinical neurological examination). Patients with ≥2 new symptoms were eligible for further diagnostics using comprehensive neuropsychological tests, cerebral MRI and 18fluorodeoxyglucose (FDG) PET as soon as infectivity was no longer present. Exclusion criteria were: premorbid diagnosis of cognitive impairment, neurodegenerative diseases or intensive care unit treatment. Of 41 COVID-19 inpatients screened, 29 patients (65.2 ± 14.4 years; 38% female) in the subacute stage of disease were included in the register. Most frequently, gustation and olfaction were disturbed in 29/29 and 25/29 patients, respectively. Montreal Cognitive Assessment performance was impaired in 18/26 patients (mean score 21.8/30) with emphasis on frontoparietal cognitive functions. This was confirmed by detailed neuropsychological testing in 15 patients. 18FDG PET revealed pathological results in 10/15 patients with predominant frontoparietal hypometabolism. This pattern was confirmed by comparison with a control sample using voxel-wise principal components analysis, which showed a high correlation (R2 = 0.62) with the Montreal Cognitive Assessment performance. Post-mortem examination of one patient revealed white matter microglia activation but no signs of neuroinflammation. Neocortical dysfunction accompanied by cognitive decline was detected in a relevant fraction of patients with subacute COVID-19 initially requiring inpatient treatment. This is of major rehabilitative and socioeconomic relevance.
Keywords: 18FDG PET; COVID-19; Montreal Cognitive Assessment; cognition; neurology.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Reply: From early limbic inflammation to long COVID sequelae.Brain. 2021 Sep 4;144(8):e66. doi: 10.1093/brain/awab216. Brain. 2021. PMID: 34142114 No abstract available.
-
From early limbic inflammation to long COVID sequelae.Brain. 2021 Sep 4;144(8):e65. doi: 10.1093/brain/awab215. Brain. 2021. PMID: 34142116 No abstract available.
References
-
- Mao L, Wang M, Chen S, et al. Neurological Manifestations of Hospitalized Patients with COVID-19 in Wuhan, China: A Retrospective Case Series Study. medRxiv [Preprint]. doi:10.1101/2020.02.22.20026500.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
