

Inhibition of the lipoxin A4 and resolvin D1 receptor impairs host response to acute lung injury caused by pneumococcal pneumonia in mice
- PMID: 33822656
- PMCID: PMC8285627
- DOI: 10.1152/ajplung.00046.2021
Inhibition of the lipoxin A4 and resolvin D1 receptor impairs host response to acute lung injury caused by pneumococcal pneumonia in mice
Abstract
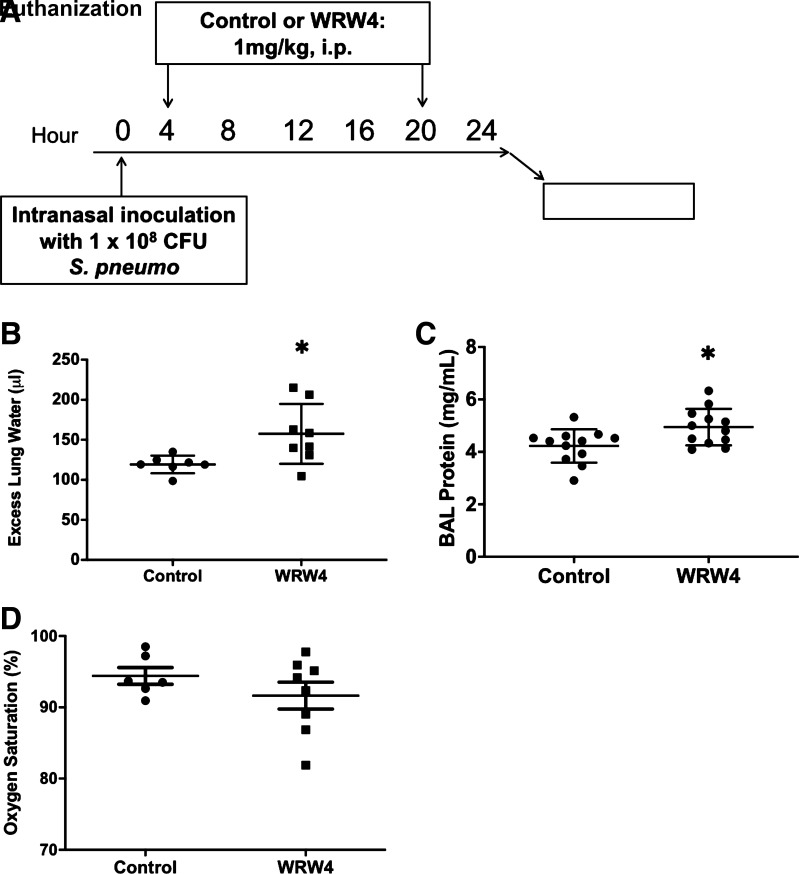
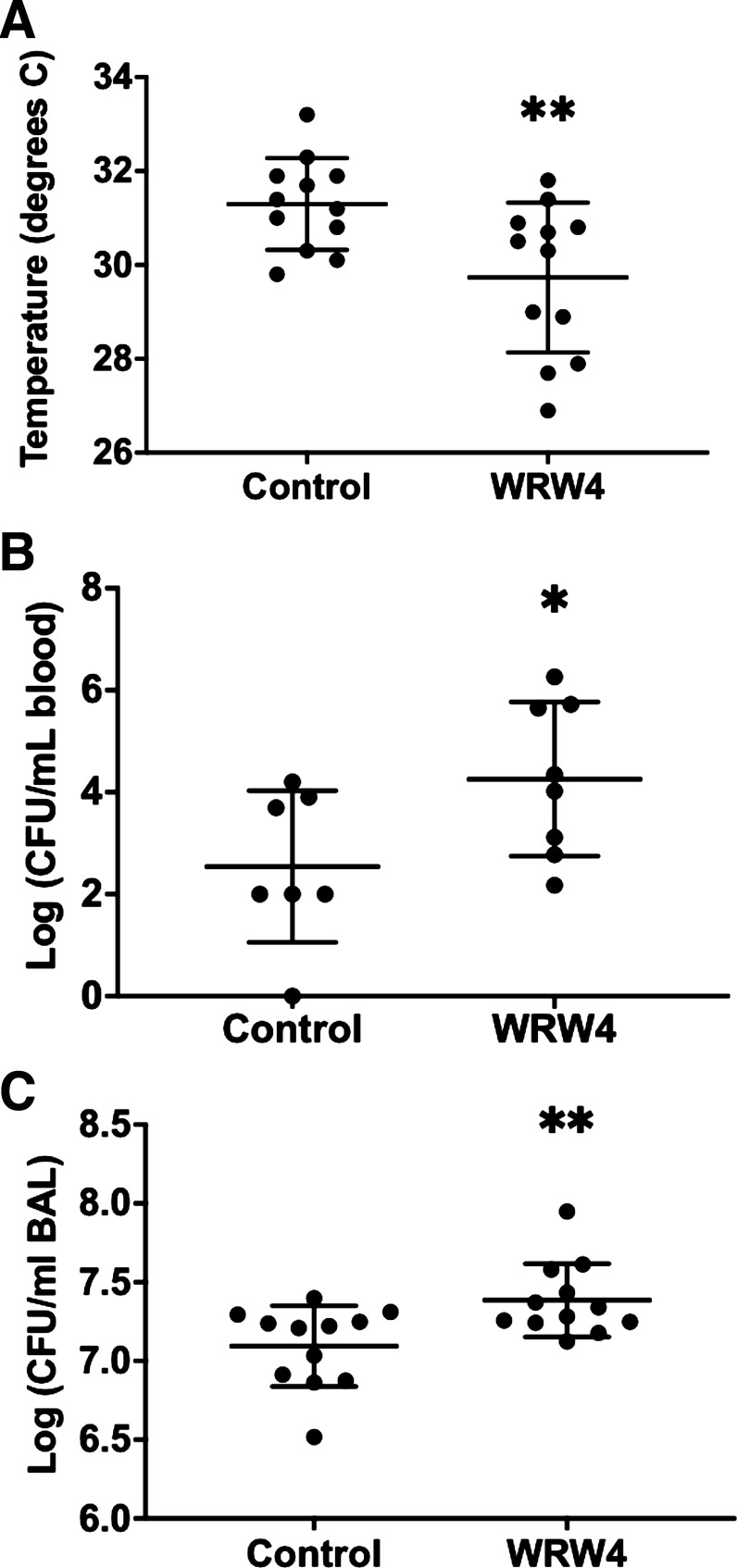
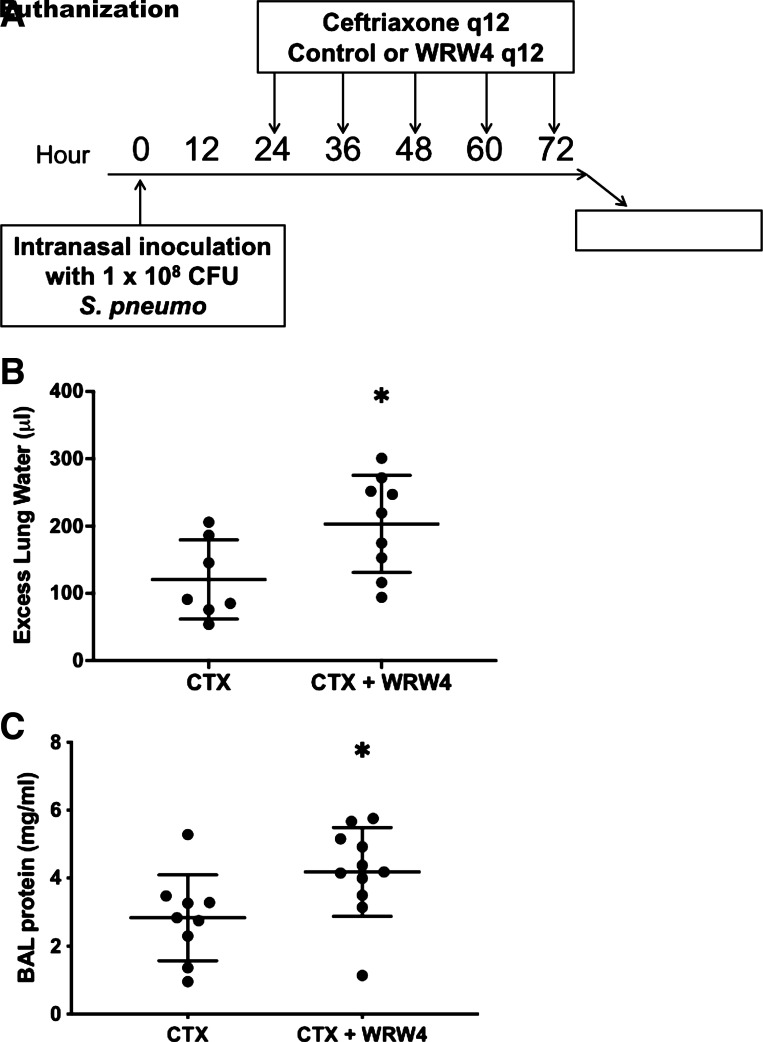
Resolution of the acute respiratory distress syndrome (ARDS) from pneumonia requires repair of the injured lung endothelium and alveolar epithelium, removal of neutrophils from the distal airspaces of the lung, and clearance of the pathogen. Previous studies have demonstrated the importance of specialized proresolving mediators (SPMs) in the regulation of host responses during inflammation. Although ARDS is commonly caused by Streptococcus pneumoniae, the role of lipoxin A4 (LXA4) and resolvin D1 (RvD1) in pneumococcal pneumonia is not well understood. In the present experimental study, we tested the hypothesis that endogenous SPMs play a role in the resolution of lung injury in a clinically relevant model of bacterial pneumonia. Blockade of formyl peptide receptor 2 (ALX/FPR2), the receptor for LXA4 and RvD1, with the peptide WRW4 resulted in more pulmonary edema, greater protein accumulation in the air spaces, and increased bacteria accumulation in the air spaces and the blood. Inhibition of this receptor was also associated with decreased levels of proinflammatory cytokines. Even in the presence of antibiotic treatment, WRW4 inhibited the resolution of lung injury. In summary, these experiments demonstrated two novel findings: LXA4 and RvD1 contribute to the resolution of lung injury due to pneumococcal pneumonia, and the mechanism of their benefit likely includes augmenting bacterial clearance and reducing pulmonary edema via the restoration of lung alveolar-capillary barrier permeability.
Keywords: ARDS; acute lung injury; infection; pneumonia; resolution.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Acute Respiratory Distress Syndrome Network; Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342: 1301–1308, 2000. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
-
- National Heart Lung and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF, Jr., Hite RD, Harabin AL. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 354: 2564–2575, 2006. doi: 10.1056/NEJMoa062200. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases