

Prevalence and characteristics of fever in adult and paediatric patients with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis of 17515 patients
- PMID: 33822812
- PMCID: PMC8023501
- DOI: 10.1371/journal.pone.0249788
Prevalence and characteristics of fever in adult and paediatric patients with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis of 17515 patients
Abstract
Background: Coronavirus disease 2019 (COVID-19), a pandemic disease caused by the severe acute respiratory syndrome coronavirus 2 started to spread globally since December 2019 from Wuhan, China. Fever has been observed as one of the most common clinical manifestations, although the prevalence and characteristics of fever in adult and paediatric COVID-19 patients is inconclusive. We aimed to conduct a systematic review and meta-analysis to estimate the overall pooled prevalence of fever and chills in addition to fever characteristics (low, medium, and high temperature) in both adult and paediatric COVID-19 patients.
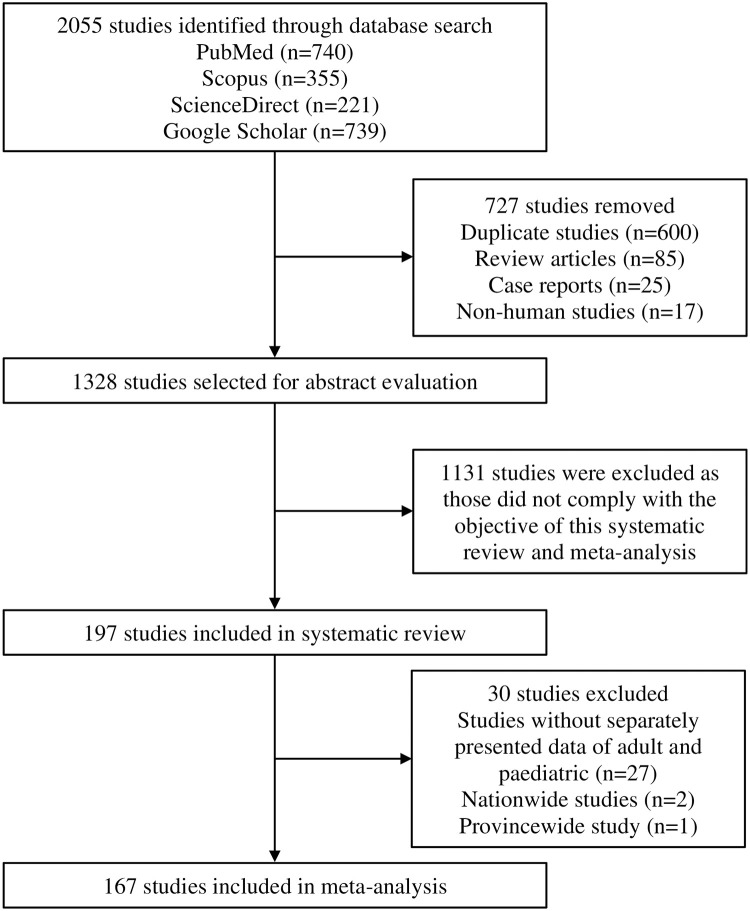
Methods: The protocol of this systematic review and meta-analysis was registered with PROSPERO (CRD42020176327). PubMed, Scopus, ScienceDirect and Google Scholar databases were searched between 1st December 2019 and 3rd April 2020 without language restrictions. Both adult (≥18 years) and paediatric (<18 years) COVID-19 patients were considered eligible. We used random-effects model for the meta-analysis to obtain the pooled prevalence and risk ratio (RR) with 95% confidence intervals (CIs). Quality assessment of included studies was performed using the Joanna Briggs Institute critical appraisal tools. Heterogeneity was assessed using the I² statistic and Cochran's Q test. Robustness of the pooled estimates was checked by different subgroups and sensitivity analyses.
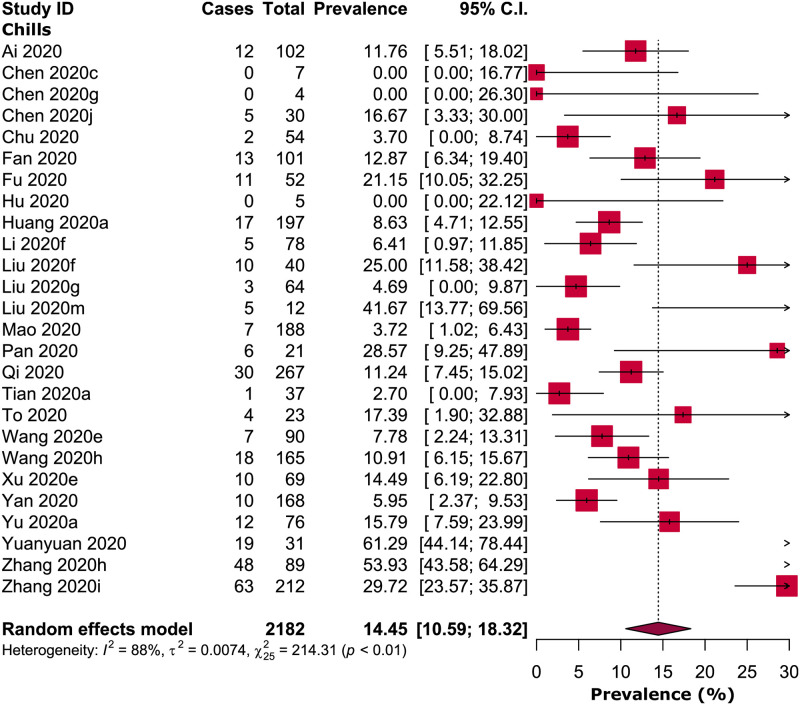
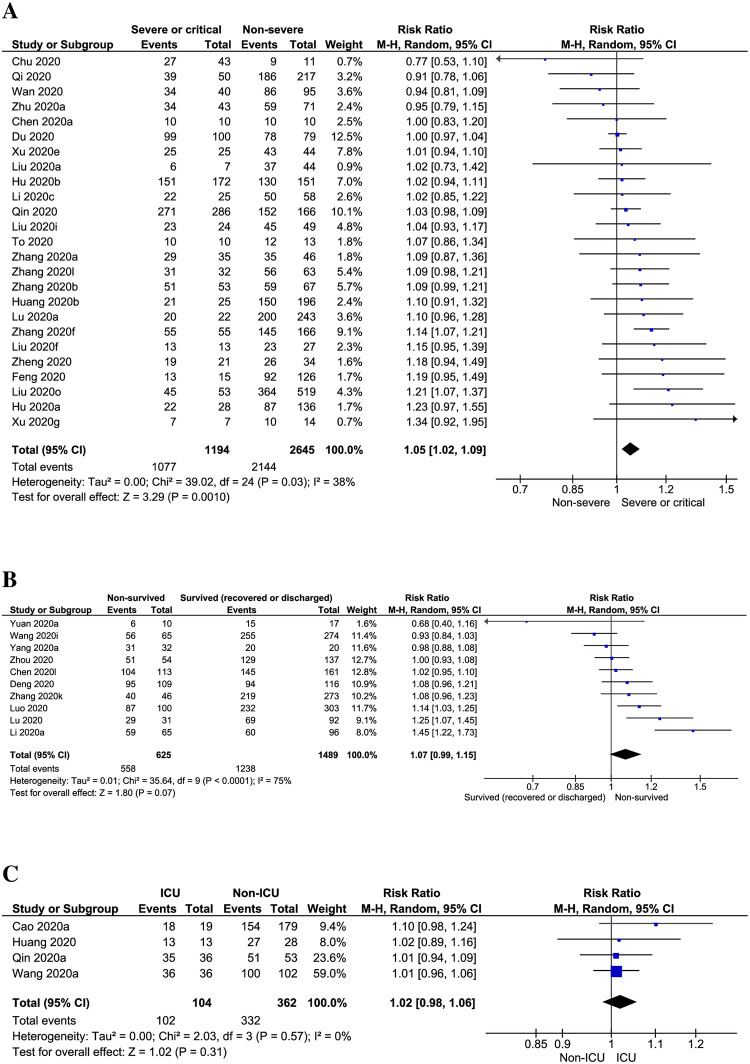
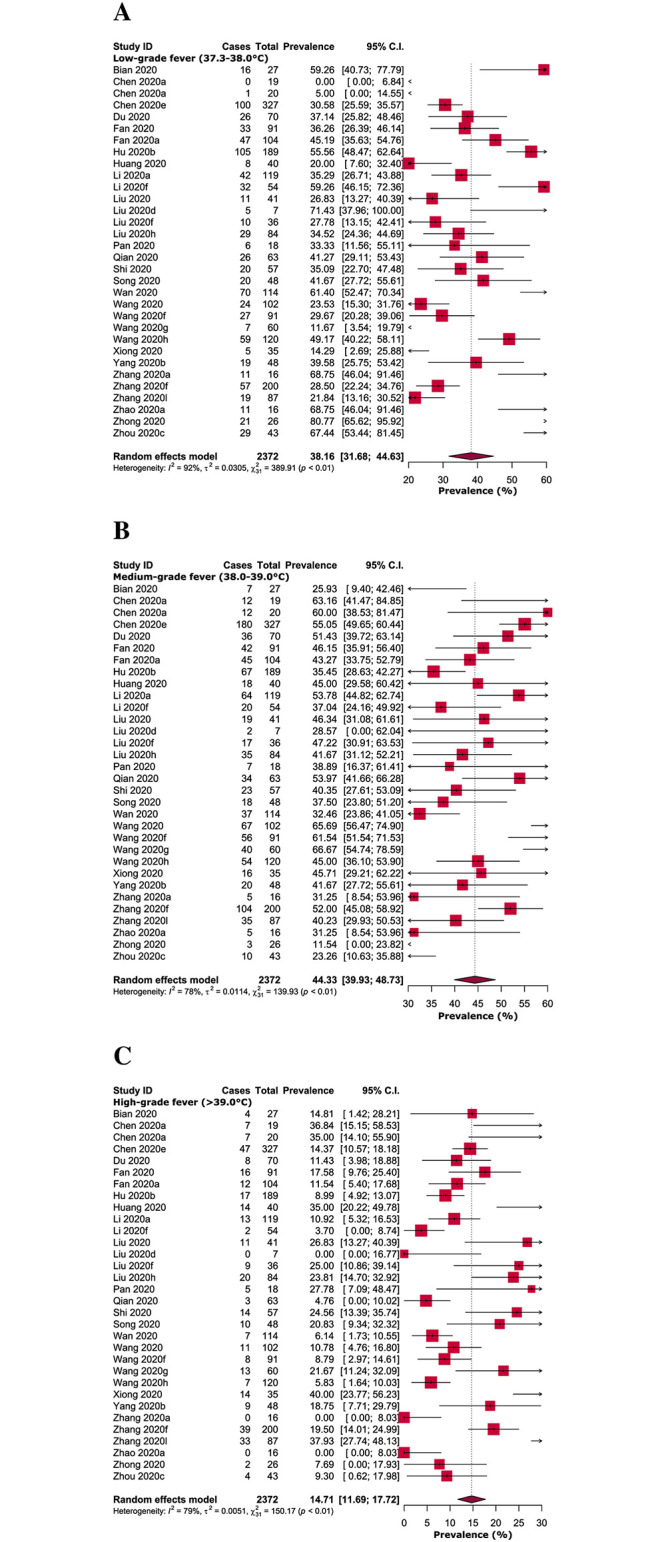
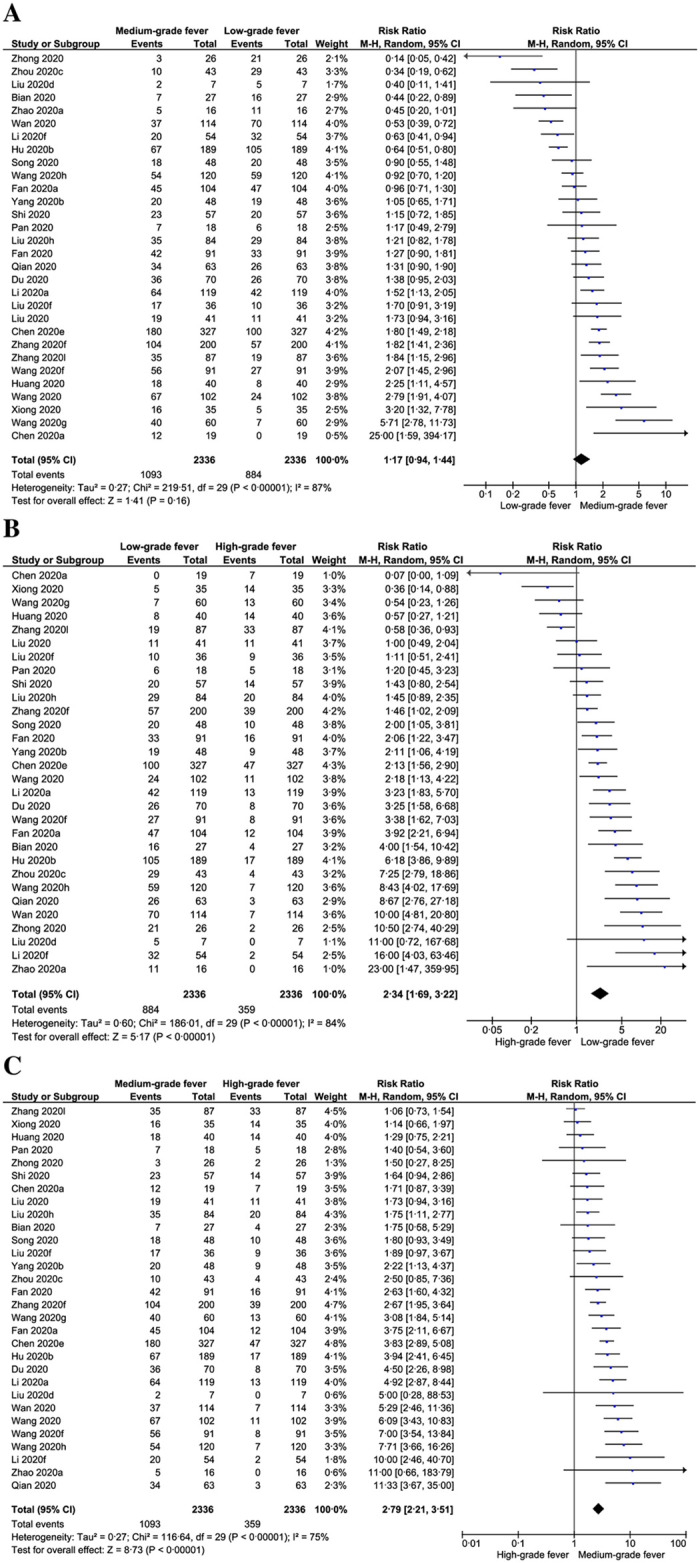
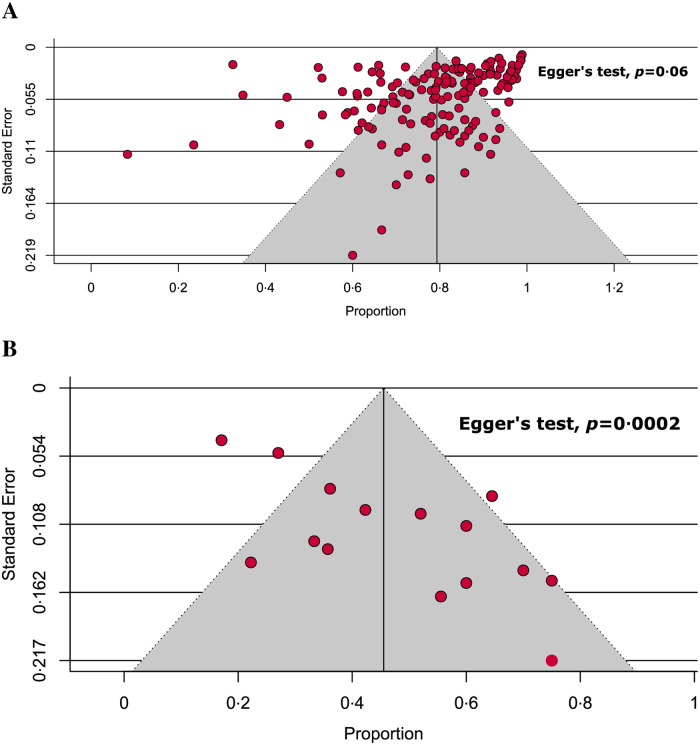
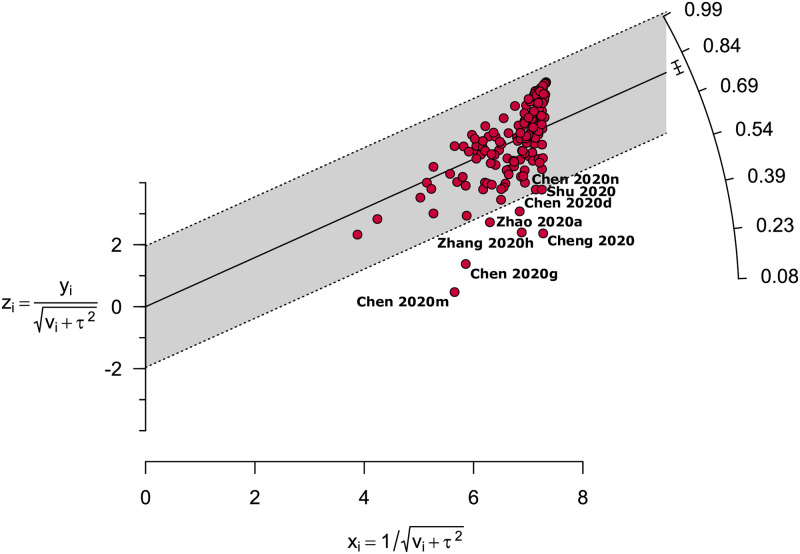
Results: We identified 2055 studies, of which 197 studies (n = 24266) were included in the systematic review and 167 studies with 17142 adults and 373 paediatrics were included in the meta-analysis. Overall, the pooled prevalence of fever in adult and paediatric COVID-19 patients were 79.43% [95% CI: 77.05-81.80, I2 = 95%] and 45.86% [95% CI: 35.24-56.48, I2 = 78%], respectively. Besides, 14.45% [95% CI: 10.59-18.32, I2 = 88%] of the adult COVID-19 patients were accompanied with chills. In adult COVID-19 patients, the prevalence of medium-grade fever (44.33%) was higher compared to low- (38.16%) and high-grade fever (14.71%). In addition, the risk of both low (RR: 2.34, 95% CI: 1.69-3.22, p<0.00001, I2 = 84%) and medium grade fever (RR: 2.79, 95% CI: 2.21-3.51, p<0.00001, I2 = 75%) were significantly higher compared to high-grade fever, however, there was no significant difference between low- and medium-grade fever (RR: 1.17, 95% CI: 0.94-1.44, p = 0.16, I2 = 87%). 88.8% of the included studies were of high-quality. The sensitivity analyses indicated that our findings of fever prevalence for both adult and paediatric patients are reliable and robust.
Conclusions: The prevalence of fever in adult COVID-19 patients was high, however, 54.14% of paediatric COVID-19 patients did not exhibit fever as an initial clinical feature. Prevalence and risk of low and medium-grade fevers were higher compared to high-grade fever.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Prevalence of Headache in Patients With Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of 14,275 Patients.Front Neurol. 2020 Nov 27;11:562634. doi: 10.3389/fneur.2020.562634. eCollection 2020. Front Neurol. 2020. PMID: 33329305 Free PMC article.
-
Clinical Features of COVID-19 Patients in the First Year of Pandemic: A Systematic Review and Meta-Analysis.Biol Res Nurs. 2022 Apr;24(2):172-185. doi: 10.1177/10998004211055866. Epub 2021 Dec 4. Biol Res Nurs. 2022. PMID: 34866409 Free PMC article.
-
Prevalence of Olfactory Dysfunction in Coronavirus Disease 2019 (COVID-19): A Meta-analysis of 27,492 Patients.Laryngoscope. 2021 Apr;131(4):865-878. doi: 10.1002/lary.29286. Epub 2020 Dec 5. Laryngoscope. 2021. PMID: 33219539 Free PMC article.
-
Prevalence and characteristics of malaria among COVID-19 individuals: A systematic review, meta-analysis, and analysis of case reports.PLoS Negl Trop Dis. 2021 Oct 1;15(10):e0009766. doi: 10.1371/journal.pntd.0009766. eCollection 2021 Oct. PLoS Negl Trop Dis. 2021. PMID: 34597315 Free PMC article.
-
Critical complications of COVID-19: A descriptive meta-analysis study.Rev Cardiovasc Med. 2020 Sep 30;21(3):433-442. doi: 10.31083/j.rcm.2020.03.129. Rev Cardiovasc Med. 2020. PMID: 33070547
Cited by
-
Angiotensin-Converting Enzyme 2 SNPs as Common Genetic Loci and Optimal Early Identification Genetic Markers for COVID-19.Pathogens. 2022 Aug 22;11(8):947. doi: 10.3390/pathogens11080947. Pathogens. 2022. PMID: 36015068 Free PMC article.
-
Post-COVID-19: Time to Change Our Way of Life for a Better Future.Epidemiologia (Basel). 2024 May 22;5(2):211-220. doi: 10.3390/epidemiologia5020015. Epidemiologia (Basel). 2024. PMID: 38804342 Free PMC article.
-
Clinical and epidemiological characteristics of influenza and SARS-CoV-2 virus among patients with acute febrile illness in selected sites of Ethiopia 2021-2022.Front Public Health. 2025 Jul 9;13:1549159. doi: 10.3389/fpubh.2025.1549159. eCollection 2025. Front Public Health. 2025. PMID: 40703157 Free PMC article.
-
Management of Children Admitted to Hospitals across Bangladesh with Suspected or Confirmed COVID-19 and the Implications for the Future: A Nationwide Cross-Sectional Study.Antibiotics (Basel). 2022 Jan 14;11(1):105. doi: 10.3390/antibiotics11010105. Antibiotics (Basel). 2022. PMID: 35052982 Free PMC article.
-
Thermal dysregulation in patients with multiple sclerosis during SARS-CoV-2 infection. The potential therapeutic role of exercise.Mult Scler Relat Disord. 2022 Mar;59:103557. doi: 10.1016/j.msard.2022.103557. Epub 2022 Jan 24. Mult Scler Relat Disord. 2022. PMID: 35092946 Free PMC article. Review.
References
-
- WHO. COVID-19 Weekly Epidemiological Update. https://www.who.int/publications/m/item/weekly-epidemiological-update—16... (accessed February 18, 2021).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
