

Heparin binding protein in severe COVID-19-A prospective observational cohort study
- PMID: 33822821
- PMCID: PMC8023466
- DOI: 10.1371/journal.pone.0249570
Heparin binding protein in severe COVID-19-A prospective observational cohort study
Abstract
Background and aims: Neutrophil-derived heparin binding protein (HBP; also known as azurocidin or CAP-37) is a key player in bacterial sepsis and a promising biomarker in severe infections. The aims of this study were to assess whether HBP is involved in the pathophysiology of COVID-19 and, if so, whether it can be used to predict severe disease preferably using a point-of-care test.
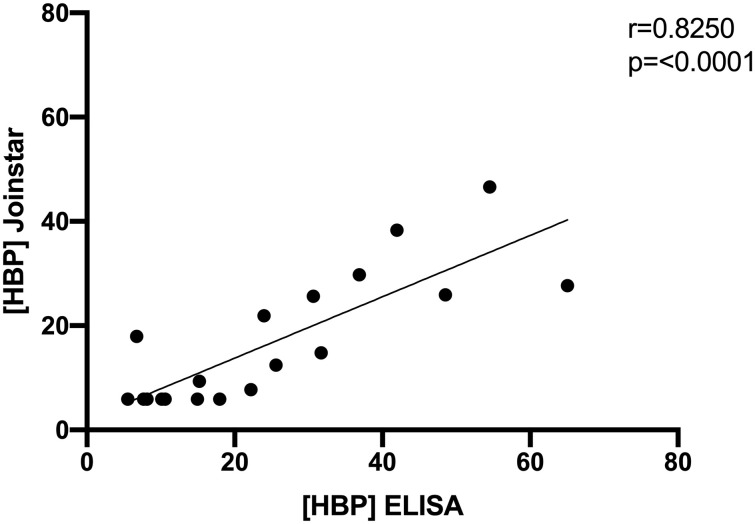
Methods: This was a prospective convenience sample study of biomarkers in patients admitted to Skåne University hospital in Sweden with a confirmed COVID-19 diagnosis. Plasma samples and clinical data were collected within 72h after admission, during hospital stay and at discharge. Plasma HBP concentrations samples were measured both with enzyme-linked immunosorbent assay (ELISA) and with a novel dry immunofluorescence analyzer (Joinstar) point-of-care test.
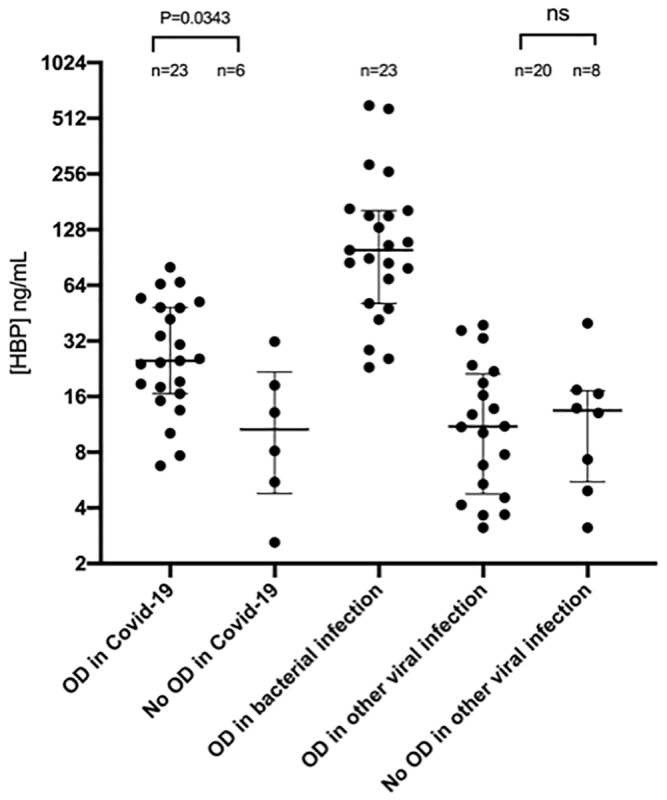
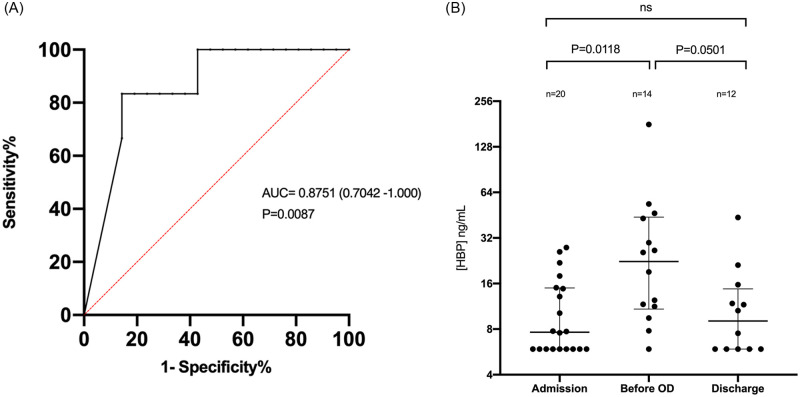
Results: Thirty-five COVID-19 patients were enrolled in the study. Twenty-nine patients had blood samples taken within 72h after admission. We compared the highest HBP value taken within 72h after admission in patients who eventually developed organ dysfunction (n = 23) compared to those who did not (n = 6), and found that HBP was significantly elevated in those who developed organ dysfunction (25.0 ng/mL (interquartile range (IQR) 16.6-48.5) vs 10.6 ng/mL (IQR 4.8-21.7 ng/mL), p = 0.03). Point-of-care test measurements correlated well with ELISA measurements (R = 0.83). HBP measured by the POC device predicted development of COVID-induced organ dysfunction with an AUC of 0.88 (95% confidence interval (CI) 0.70-1.0).
Conclusions: HBP is elevated prior to onset of organ dysfunction in patients with severe COVID-19 using a newly developed point-of-care test and hence HBP could be used in a clinical setting as a prognostic marker in COVID-19.
Conflict of interest statement
Adam Linder is listed as inventors on a patent on the use of HBP as a diagnostic tool in sepsis filed by Hansa Medical AB WO2008151808A1. This does not alter our adherence to PLOS ONE policies on sharing data and materials. All other authors have declared no relevant conflicts of interest.
Figures
Similar articles
-
Elevated plasma levels of heparin-binding protein in intensive care unit patients with severe sepsis and septic shock.Crit Care. 2012 May 21;16(3):R90. doi: 10.1186/cc11353. Crit Care. 2012. PMID: 22613179 Free PMC article.
-
Heparin Binding Protein in Adult Heart Surgery.Ann Thorac Surg. 2019 Apr;107(4):1154-1159. doi: 10.1016/j.athoracsur.2018.10.007. Epub 2018 Nov 14. Ann Thorac Surg. 2019. PMID: 30447193
-
Integration of heparin-binding protein and interleukin-6 in the early prediction of respiratory failure and mortality in pneumonia by SARS-CoV-2 (COVID-19).Eur J Clin Microbiol Infect Dis. 2021 Jul;40(7):1405-1412. doi: 10.1007/s10096-020-04145-7. Epub 2021 Jan 29. Eur J Clin Microbiol Infect Dis. 2021. PMID: 33515095 Free PMC article.
-
Heparin-binding protein: a key player in the pathophysiology of organ dysfunction in sepsis.J Intern Med. 2017 Jun;281(6):562-574. doi: 10.1111/joim.12604. Epub 2017 Mar 28. J Intern Med. 2017. PMID: 28370601 Review.
-
Diagnostic and prognostic value of heparin-binding protein in sepsis: A systematic review and meta-analysis.Medicine (Baltimore). 2024 Jun 21;103(25):e38525. doi: 10.1097/MD.0000000000038525. Medicine (Baltimore). 2024. PMID: 38905400 Free PMC article.
Cited by
-
Hematologic cancers and infections: how to detect infections in advance and determine the type?Front Cell Infect Microbiol. 2024 Nov 4;14:1476543. doi: 10.3389/fcimb.2024.1476543. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39559703 Free PMC article. Review.
-
Neutrophil Extracellular Traps, Sepsis and COVID-19 - A Tripod Stand.Front Immunol. 2022 Jun 10;13:902206. doi: 10.3389/fimmu.2022.902206. eCollection 2022. Front Immunol. 2022. PMID: 35757734 Free PMC article. Review.
-
Heparin-binding Protein as a Diagnostic and Prognostic Marker of Infections: A Systematic Review and Meta-analysis.Mediterr J Hematol Infect Dis. 2025 May 1;17(1):e2025029. doi: 10.4084/MJHID.2025.029. eCollection 2025. Mediterr J Hematol Infect Dis. 2025. PMID: 40375914 Free PMC article. Review.
-
Antimicrobial Mechanisms and Clinical Application Prospects of Antimicrobial Peptides.Molecules. 2022 Apr 21;27(9):2675. doi: 10.3390/molecules27092675. Molecules. 2022. PMID: 35566025 Free PMC article. Review.
-
Reference Interval for the Axis-Shield Clinical Chemistry Heparin-Binding Protein Assay.Diagnostics (Basel). 2022 Aug 10;12(8):1930. doi: 10.3390/diagnostics12081930. Diagnostics (Basel). 2022. PMID: 36010280 Free PMC article.
References
-
- (WHO) WHO (2020) Coronavirus disease 2019 (COVID-19): situation report. World Health Organization 209.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
