

Characterizing physician EHR use with vendor derived data: a feasibility study and cross-sectional analysis
- PMID: 33822970
- PMCID: PMC8279798
- DOI: 10.1093/jamia/ocab011
Characterizing physician EHR use with vendor derived data: a feasibility study and cross-sectional analysis
Abstract
Objective: To derive 7 proposed core electronic health record (EHR) use metrics across 2 healthcare systems with different EHR vendor product installations and examine factors associated with EHR time.
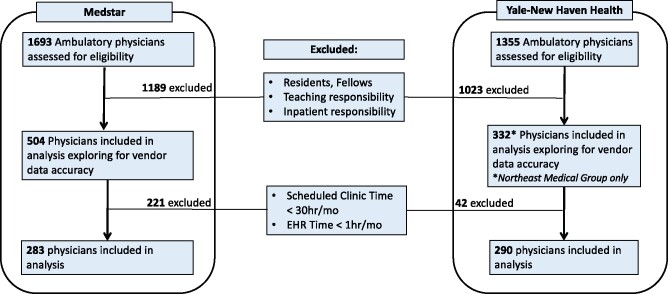
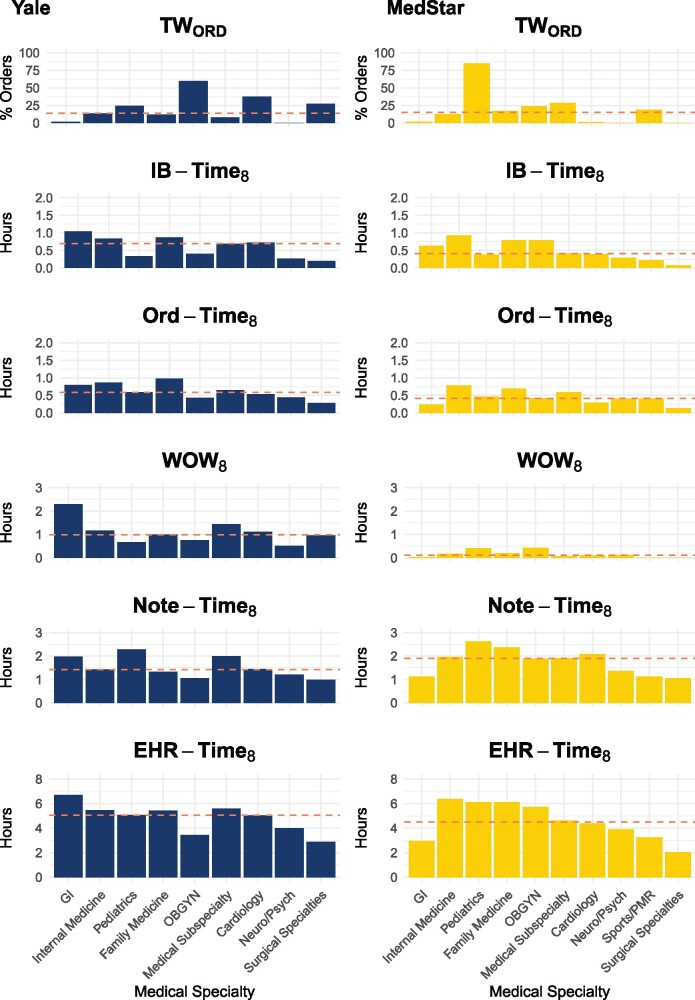
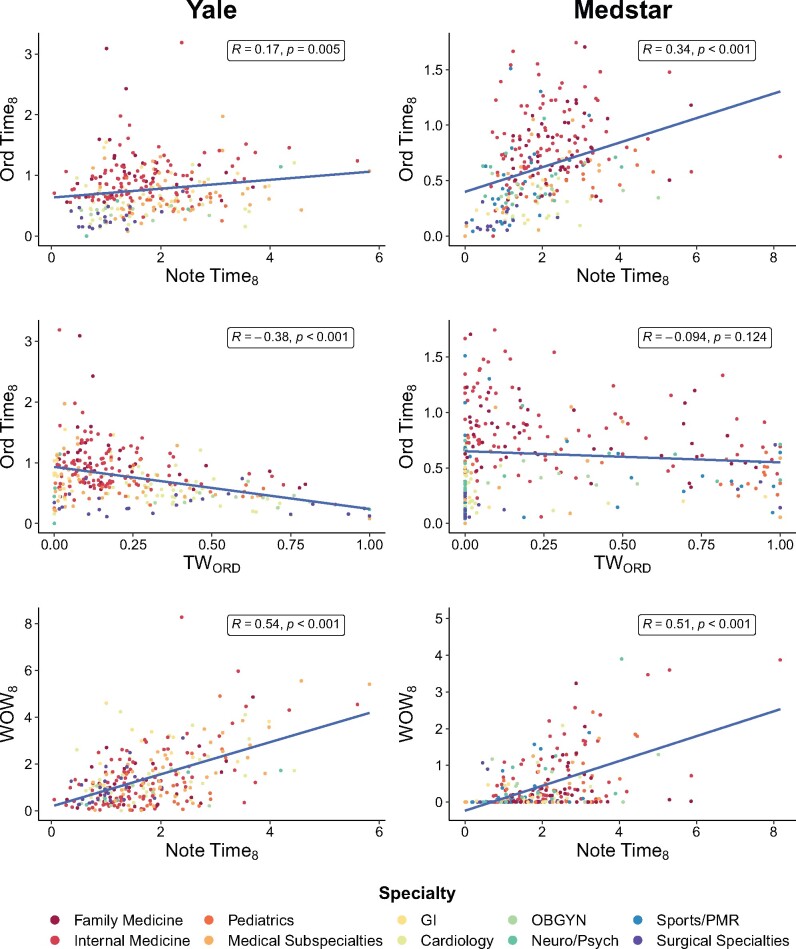
Materials and methods: A cross-sectional analysis of ambulatory physicians EHR use across the Yale-New Haven and MedStar Health systems was performed for August 2019 using 7 proposed core EHR use metrics normalized to 8 hours of patient scheduled time.
Results: Five out of 7 proposed metrics could be measured in a population of nonteaching, exclusively ambulatory physicians. Among 573 physicians (Yale-New Haven N = 290, MedStar N = 283) in the analysis, median EHR-Time8 was 5.23 hours. Gender, additional clinical hours scheduled, and certain medical specialties were associated with EHR-Time8 after adjusting for age and health system on multivariable analysis. For every 8 hours of scheduled patient time, the model predicted these differences in EHR time (P < .001, unless otherwise indicated): female physicians +0.58 hours; each additional clinical hour scheduled per month -0.01 hours; practicing cardiology -1.30 hours; medical subspecialties -0.89 hours (except gastroenterology, P = .002); neurology/psychiatry -2.60 hours; obstetrics/gynecology -1.88 hours; pediatrics -1.05 hours (P = .001); sports/physical medicine and rehabilitation -3.25 hours; and surgical specialties -3.65 hours.
Conclusions: For every 8 hours of scheduled patient time, ambulatory physicians spend more than 5 hours on the EHR. Physician gender, specialty, and number of clinical hours practicing are associated with differences in EHR time. While audit logs remain a powerful tool for understanding physician EHR use, additional transparency, granularity, and standardization of vendor-derived EHR use data definitions are still necessary to standardize EHR use measurement.
© The Author(s) 2021. Published by Oxford University Press on behalf of the American Medical Informatics Association.
Figures
References
-
- Ratwani RM, Savage E, Will A, et al.Identifying electronic health record usability and safety challenges in pediatric settings. Health Aff 2018; 37 (11): 1752–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
