

Clinical features, neurologic recovery, and risk factors of postoperative posterior fossa syndrome and delayed recovery: a prospective study
- PMID: 33823018
- PMCID: PMC8408840
- DOI: 10.1093/neuonc/noab030
Clinical features, neurologic recovery, and risk factors of postoperative posterior fossa syndrome and delayed recovery: a prospective study
Abstract
Background: Posterior fossa syndrome (PFS) is a known consequence of medulloblastoma resection. Our aim was to clinically define PFS, its evolution over time, and ascertain risk factors for its development and poor recovery.
Methods: Children with medulloblastoma treated at St Jude Children's Research Hospital from 6/2013 to 7/2019 received standardized neurological examinations, before and periodically after radiation therapy. Most (98.3%) were enrolled on the ongoing multi-institutional protocol (SJMB12; NCT01878617).
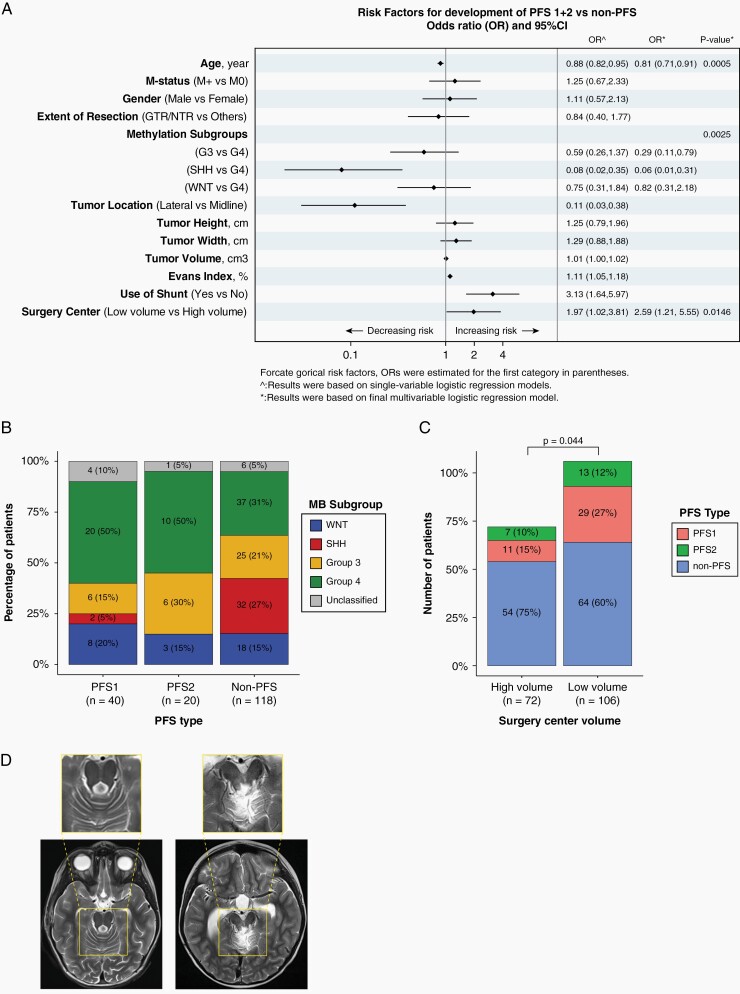
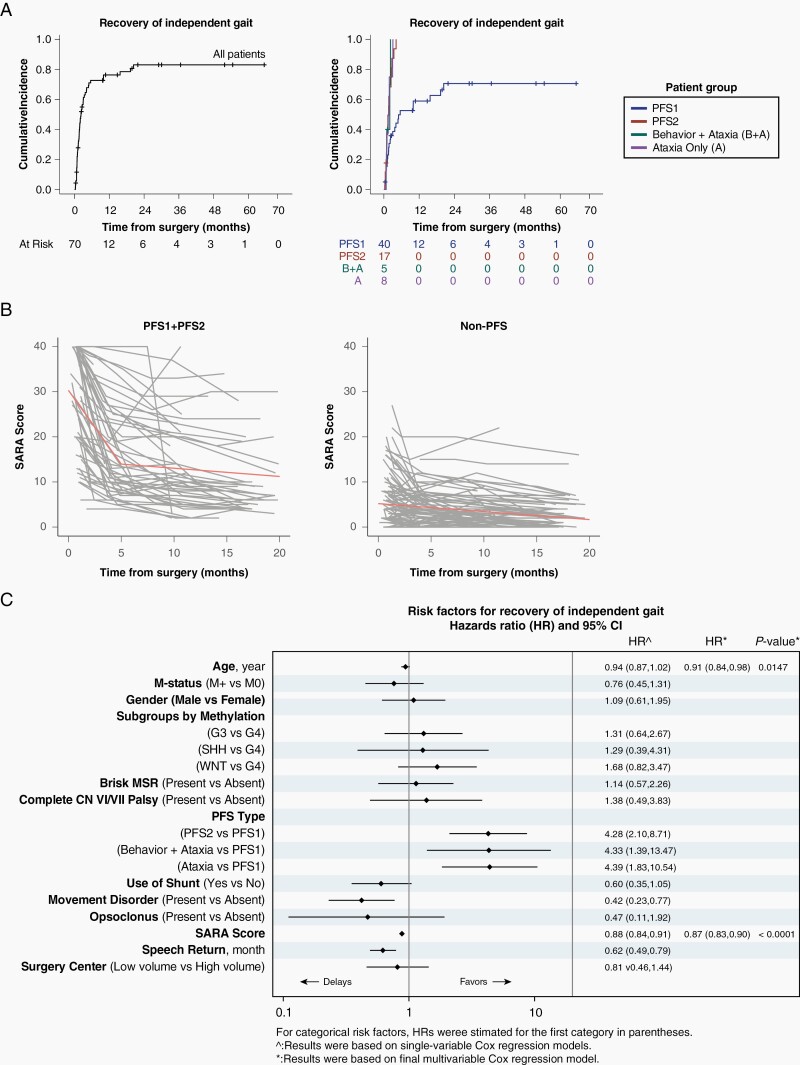
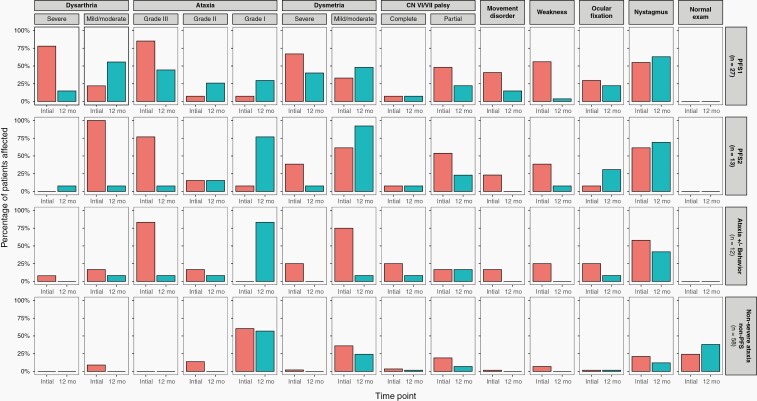
Results: Sixty (34%) of 178 evaluated children had PFS. Forty (23%) had complete mutism (PFS1) and 20 (11%) had diminished speech (PFS2). All children with PFS had severe ataxia and 42.5% of PFS1 had movement disorders. By multivariable analysis, younger age (P = .0005) and surgery in a low-volume surgery center (P = .0146) increased PFS risk, while Sonic Hedgehog tumors had reduced risk (P = .0025). Speech and gait returned in PFS1/PFS2 children at a median of 2.3/0.7 and 2.1/1.5 months, respectively, however, 12 (44.4%) of 27 PFS1 children with 12 months of follow-up were nonambulatory at 1 year. Movement disorder (P = .037) and high ataxia score (P < .0001) were associated with delayed speech recovery. Older age (P = .0147) and high ataxia score (P < .0001) were associated with delayed gait return. Symptoms improved in all children but no child with PFS had normal neurologic examination at a median of 23 months after surgery.
Conclusions: Categorizing PFS into types 1 and 2 has prognostic relevance. Almost half of the children with PFS1 with 12-month follow-up were nonambulatory. Surgical experience was a major modifiable contributor to the development of PFS.
Keywords: cerebellar mutism; medulloblastoma; outcome; posterior fossa syndrome; risk factors.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Posterior fossa syndrome-time to unmute the silence on cerebellar mutism.Neuro Oncol. 2021 Sep 1;23(9):1427-1428. doi: 10.1093/neuonc/noab147. Neuro Oncol. 2021. PMID: 34139019 Free PMC article. No abstract available.
References
-
- Robertson PL, Muraszko KM, Holmes EJ, et al. ; Children’s Oncology Group . Incidence and severity of postoperative cerebellar mutism syndrome in children with medulloblastoma: a prospective study by the Children’s Oncology Group. J Neurosurg. 2006;105(6 Suppl):444–451. - PubMed
-
- Gudrunardottir T, Sehested A, Juhler M, Schmiegelow K. Cerebellar mutism: review of the literature. Childs Nerv Syst. 2011;27(3):355–363. - PubMed
-
- Tamburrini G, Frassanito P, Chieffo D, Massimi L, Caldarelli M, Di Rocco C. Cerebellar mutism. Childs Nerv Syst. 2015;31(10):1841–1851. - PubMed
-
- Gudrunardottir T, Morgan AT, Lux AL, et al. ; Iceland Delphi Group . Consensus paper on post-operative pediatric cerebellar mutism syndrome: the Iceland Delphi results. Childs Nerv Syst. 2016;32(7):1195–1203. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
