

Evolution in the Presentation, Treatment, and Outcomes of Patients with Acute Mesenteric Ischemia
- PMID: 33823263
- PMCID: PMC8349780
- DOI: 10.1016/j.avsg.2021.01.116
Evolution in the Presentation, Treatment, and Outcomes of Patients with Acute Mesenteric Ischemia
Abstract
Objectives: Acute mesenteric ischemia (AMI) is a life-threatening condition associated with dismal outcomes. This study sought to evaluate the evolution of presentation, treatment, and outcomes of AMI over the past two decades.
Methods: AMI patients presenting at a single institution were reviewed (1993-2016). Venous thrombosis patients were excluded. Primary outcome was 30-day mortality. Patients were stratified by etiology and diagnosis date (before 2004 versus 2004 and later). Ordered logistic regression was performed for longitudinal temporal analysis.
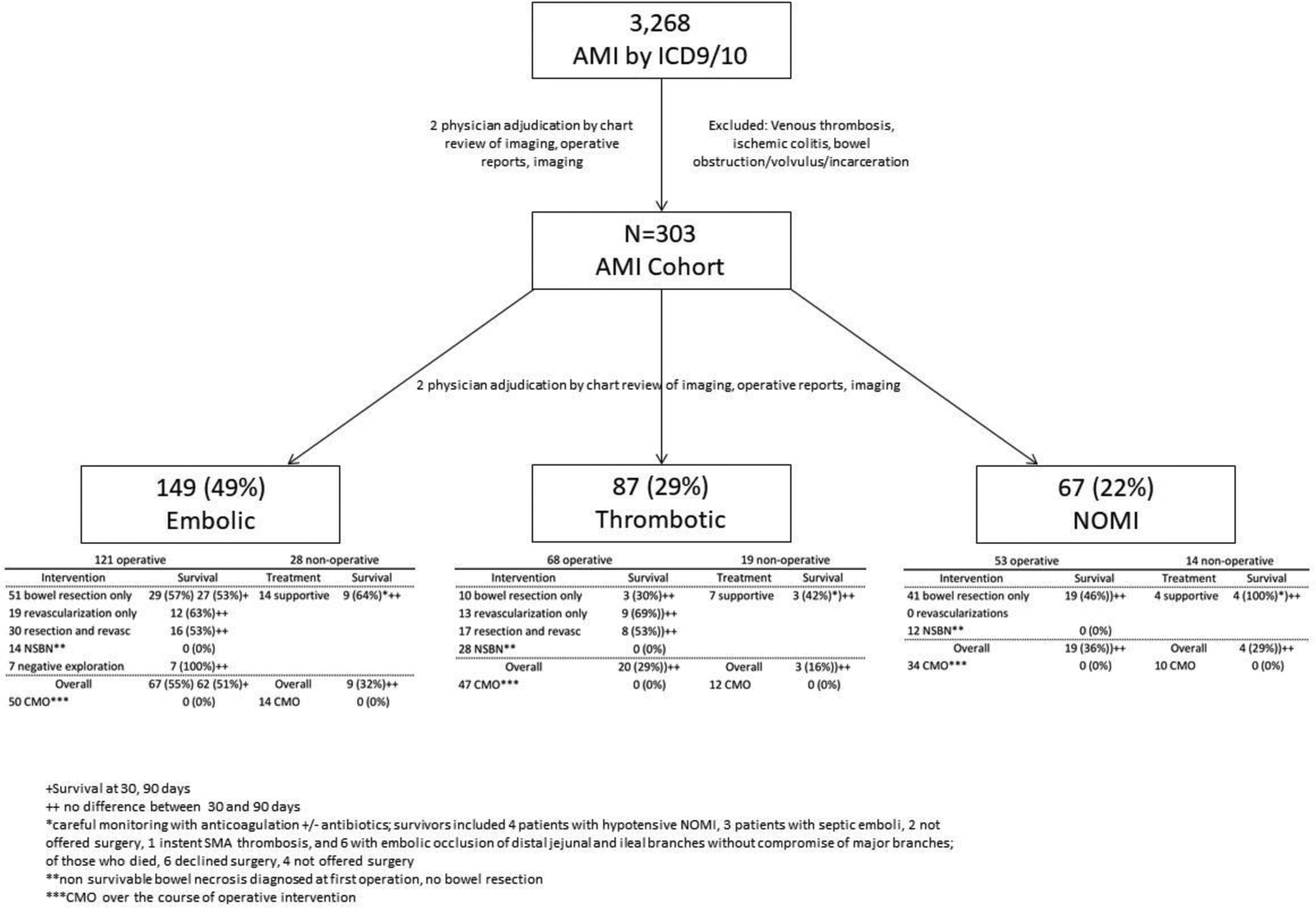
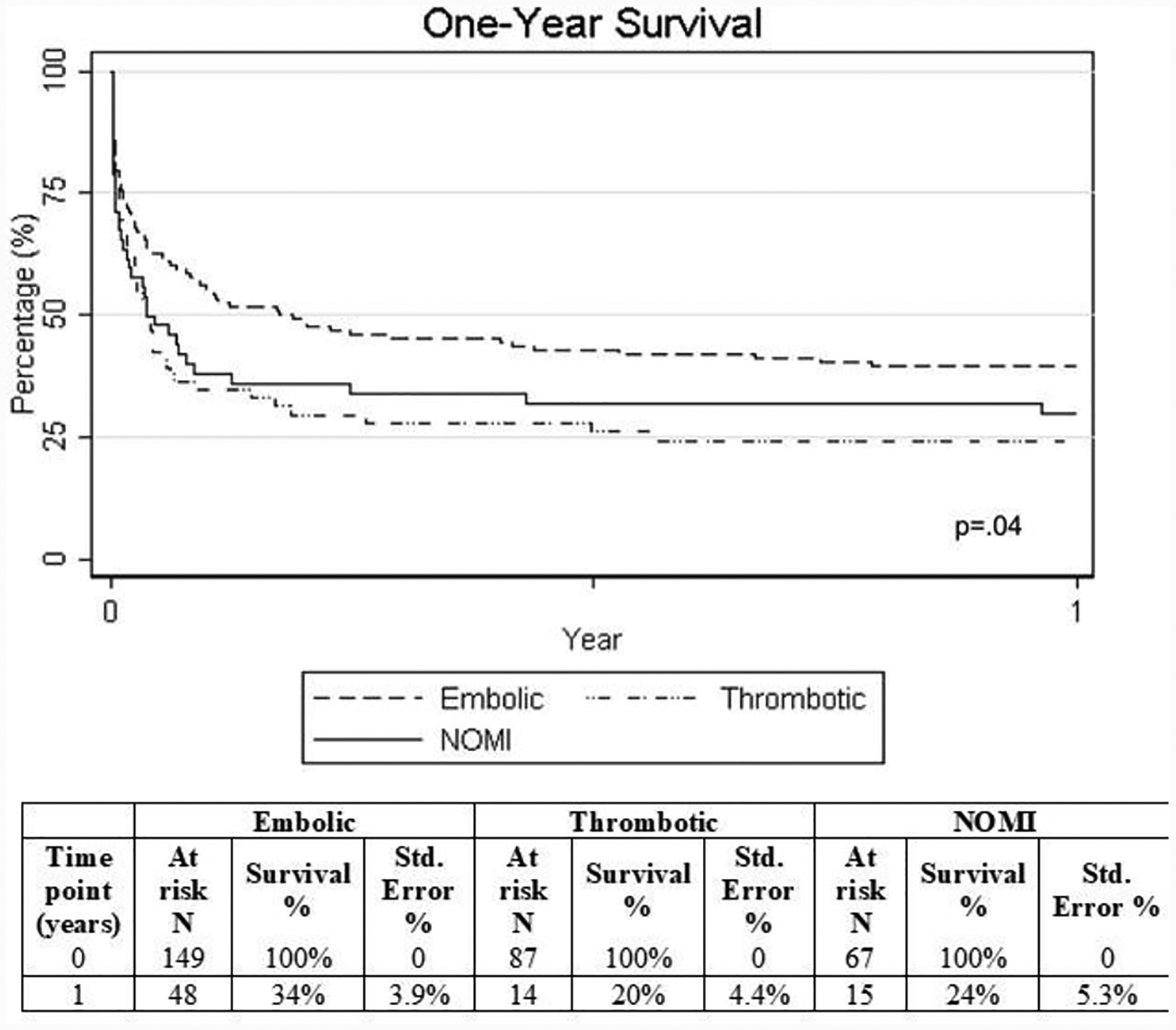
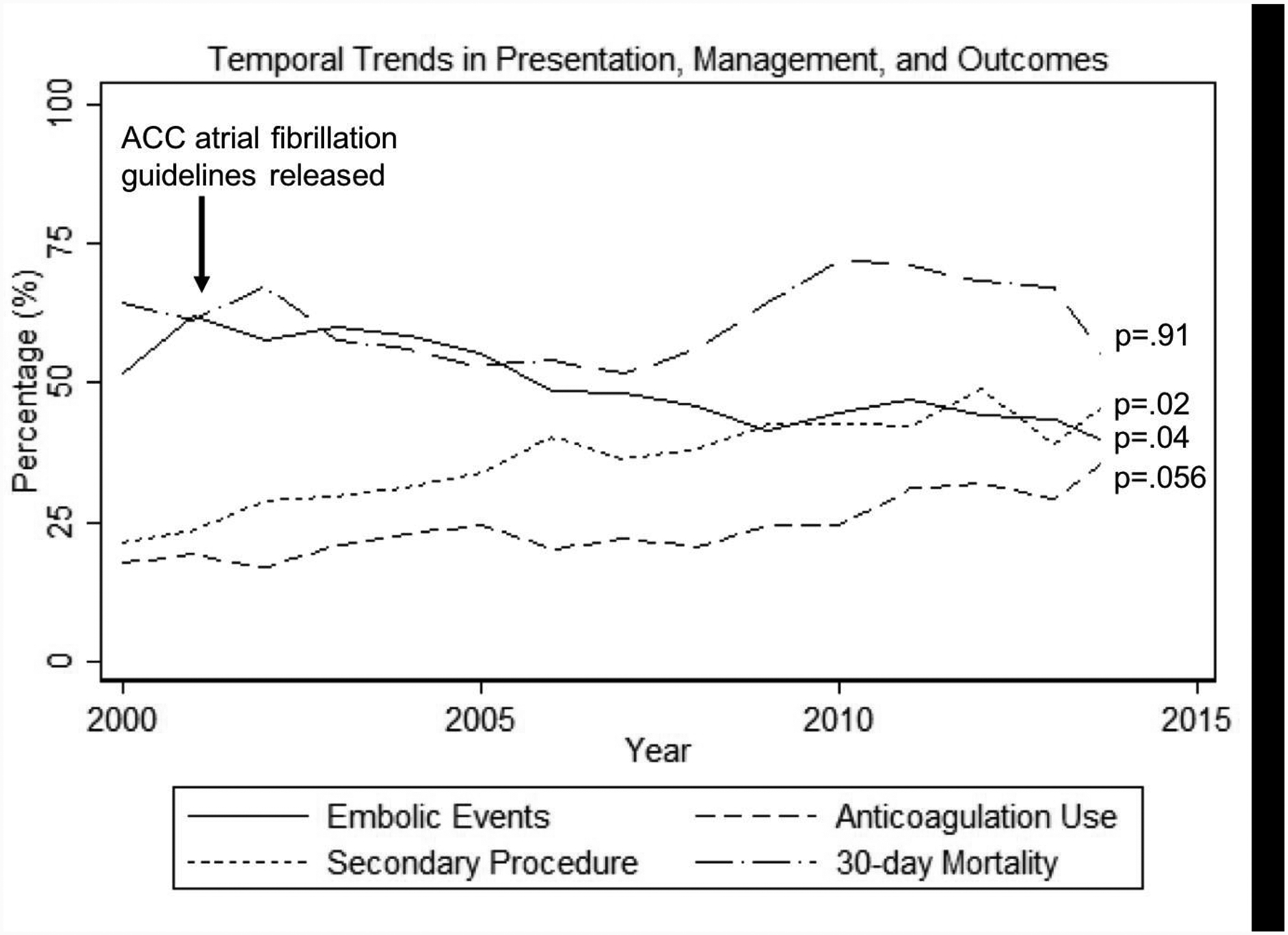
Results: 303 patients were identified. AMI mechanisms included: embolic (49%), thrombotic (29%), and non-occlusive (NOMI) (22%). The majority were women (55%), 50% had atrial fibrillation, and 23% were on anticoagulation (AC) therapy. Mean age was 72±13 years. 345 procedures were performed in 242 patients: 321 open and 24 hybrid/endovascular. Among the 189 embolic/thrombotic patients who were managed operatively, 45% (n=85) underwent mesenteric revascularization while 39 (21%) had findings of non-survivable bowel necrosis (NSBN). Among the 104 patients who did not undergo revascularization, 64 (62%) died within 30-days compared to 36 out of 85 (42%) patients who were revascularized (P=0.01). 30-day mortality was 61% and stable over time (P=0.91); when stratified by AMI etiology, the thrombotic cohort had worse survival than embolic and NOMI patients (P=0.04). Since 2000, there was a significant decrease in the percentage of embolic AMI events (P=0.04). The percentage of patients who underwent operative management decreased also over time (P=0.01, 81% → 61%), which was correlated with an increasing number of patients being made comfort measures only (CMO) prior to surgical intervention (50% → 70%, P=0.02). The majority of patients (55%) were ultimately made CMO during their hospitalization. Predictors of 30-day mortality included a preoperative white blood cell count (WBC) ≥ 25 K/ µL. (OR 3.0, P=0.002) and lactate ≥ 2.3 mmol/L (OR 2.8, P=0.045). NSBN predictors included WBC ≥ 24 K/ µL. (OR 3.4 P=0.03) and lactate ≥ 3.8 mmol/L (OR 3.6, P=0.04).
Conclusions: Despite advances in critical care over the past 25 years, AMI continues to be associated with poor prognosis. The survival benefit observed in patients who undergo revascularization supports an aggressive approach towards early vascular intervention, although this requires further study. The importance of early diagnosis, prognostication and advanced directives is highlighted given the high morbidity, mortality and use of comfort measures associated with AMI.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Figures
Similar articles
-
Endovascular Revascularization with Stent Implantation in Patients with Acute Mesenteric Ischemia due to Acute Arterial Thrombosis: Clinical Outcome and Predictive Factors.Cardiovasc Intervent Radiol. 2021 Jul;44(7):1030-1038. doi: 10.1007/s00270-021-02824-2. Epub 2021 Apr 6. Cardiovasc Intervent Radiol. 2021. PMID: 33825061 Free PMC article.
-
Thirty-Day Outcomes After Open Revascularization for Acute Mesenteric Ischemia From the American College of Surgeons National Surgical Quality Improvement Program.Ann Vasc Surg. 2019 Nov;61:148-155. doi: 10.1016/j.avsg.2019.05.024. Epub 2019 Aug 2. Ann Vasc Surg. 2019. PMID: 31382003
-
Outcomes of antegrade and retrograde open mesenteric bypass for acute mesenteric ischemia.J Vasc Surg. 2019 Jan;69(1):129-140. doi: 10.1016/j.jvs.2018.04.063. Epub 2018 Jun 29. J Vasc Surg. 2019. PMID: 30580778
-
Contemporary management of acute mesenteric ischemia: Factors associated with survival.J Vasc Surg. 2002 Mar;35(3):445-52. doi: 10.1067/mva.2002.120373. J Vasc Surg. 2002. PMID: 11877691 Review.
-
Contemporary Management of Acute Mesenteric Ischemia in the Endovascular Era.Vasc Endovascular Surg. 2019 Jan;53(1):42-50. doi: 10.1177/1538574418805228. Epub 2018 Oct 25. Vasc Endovascular Surg. 2019. PMID: 30360689 Review.
Cited by
-
Acute Mesenteric Ischemia Secondary to Candida Endocarditis: A Case Report.Cureus. 2024 Mar 22;16(3):e56747. doi: 10.7759/cureus.56747. eCollection 2024 Mar. Cureus. 2024. PMID: 38523876 Free PMC article.
-
Complex case of acute mesenteric ischemia in a patient with atrial fibrillation: A radiologic -surgical collaboration for timely intervention.Bioinformation. 2024 Dec 31;20(12):1922-1926. doi: 10.6026/9732063002001922. eCollection 2024. Bioinformation. 2024. PMID: 40230934 Free PMC article.
-
Acute Mesenteric Ischemia: Preexisting Comorbidity Determines Short-Term Outcome and Quality of Life in Long-Term Survivors.Visc Med. 2022 Dec;38(6):393-399. doi: 10.1159/000526921. Epub 2022 Nov 24. Visc Med. 2022. PMID: 36589248 Free PMC article.
-
Acute mesenteric ischemia: updated guidelines of the World Society of Emergency Surgery.World J Emerg Surg. 2022 Oct 19;17(1):54. doi: 10.1186/s13017-022-00443-x. World J Emerg Surg. 2022. PMID: 36261857 Free PMC article. Review.
-
Incidence and outcomes of acute mesenteric ischaemia: a systematic review and meta-analysis.BMJ Open. 2022 Oct 25;12(10):e062846. doi: 10.1136/bmjopen-2022-062846. BMJ Open. 2022. PMID: 36283747 Free PMC article.
References
-
- Kassahun WT, Schulz T, Richter O, Hauss J. Unchanged high mortality rates from acute occlusive intestinal ischemia: Six year review. Langenbecks Arch Surg. 2008;393:163–171 - PubMed
-
- Nuzzo A, Maggiori L, Ronot M, Becq A, Plessier A, Gault N, et al. Predictive factors of intestinal necrosis in acute mesenteric ischemia: Prospective study from an intestinal stroke center. Am J Gastroenterol. 2017;112:597–605 - PubMed
-
- Karkkainen JM, Lehtimaki TT, Manninen H, Paajanen H. Acute mesenteric ischemia is a more common cause than expected of acute abdomen in the elderly. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2015;19:1407–1414 - PubMed
-
- Stoney RJ, Cunningham CG. Acute mesenteric ischemia. Surgery. 1993;114:489–490 - PubMed
-
- Fuster V, Ryden LE, Asinger RW, Cannom DS, Crijns HJ, Frye RL, et al. Acc/aha/esc guidelines for the management of patients with atrial fibrillation: Executive summary a report of the american college of cardiology/american heart association task force on practice guidelines and the european society of cardiology committee for practice guidelines and policy conferences (committee to develop guidelines for the management of patients with atrial fibrillation) developed in collaboration with the north american society of pacing and electrophysiology. Circulation. 2001;104:2118–2150 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
