

Effectiveness of P-wave ECG index and left atrial appendage volume in predicting atrial fibrillation recurrence after first radiofrequency catheter ablation
- PMID: 33823799
- PMCID: PMC8022391
- DOI: 10.1186/s12872-021-01930-w
Effectiveness of P-wave ECG index and left atrial appendage volume in predicting atrial fibrillation recurrence after first radiofrequency catheter ablation
Abstract
Background: The primary aim was to observe the predictive value of P-wave ECG index and left atrial appendage volume (LLAV) for atrial fibrillation recurrence after first radiofrequency catheter ablation.
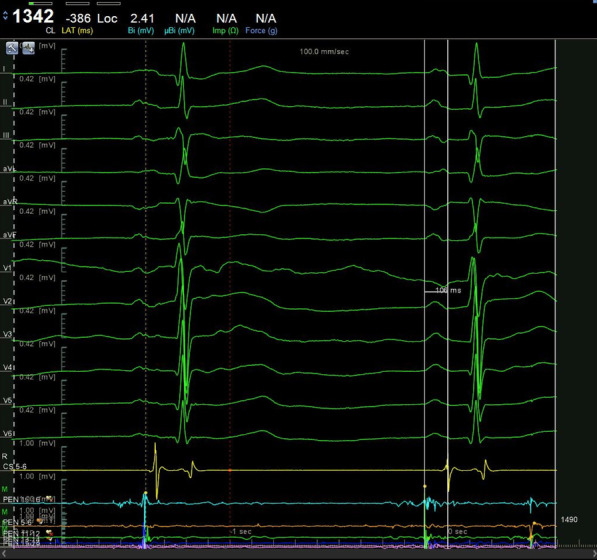
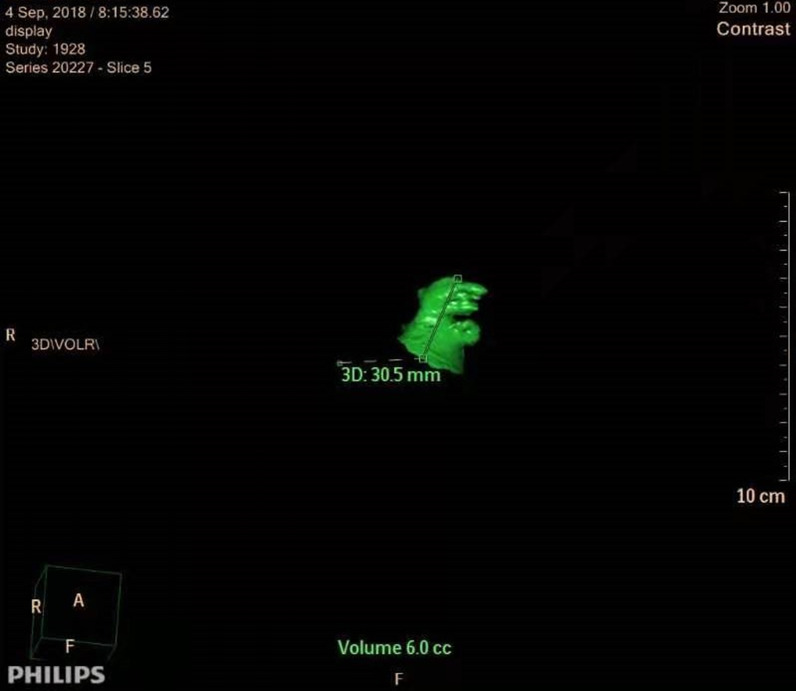
Methods: A total of 196 patients with paroxysmal atrial fibrillation were enrolled. The preoperative LLAV was measured by cardiac enhanced CT. The P-wave ECG index including minimum P-wave duration (P-min), maximum P-wave duration (P-max), mean P-wave duration (mPWD), P-wave dispersion (PWD), P-wave terminal force in lead V1 (PtfV1), PR interval prolongation, and interatrial block (IAB) were analyzed and recorded in 12-lead ECG of sinus rhythm.
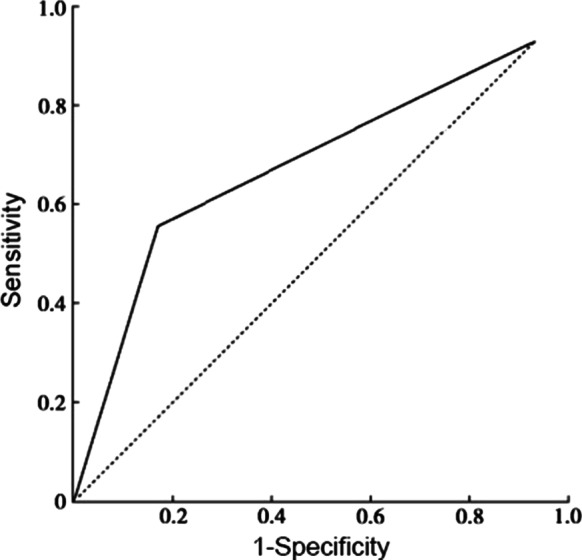
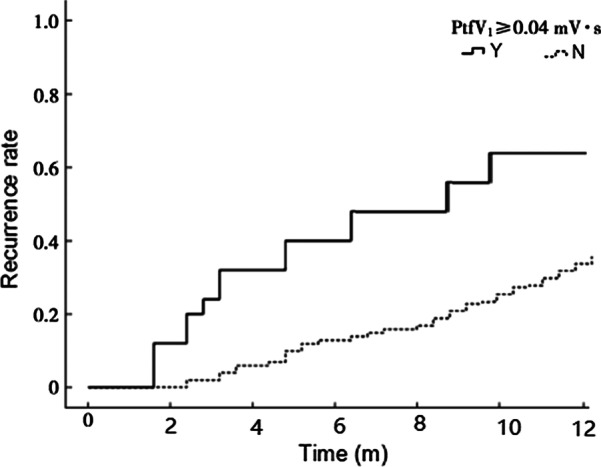
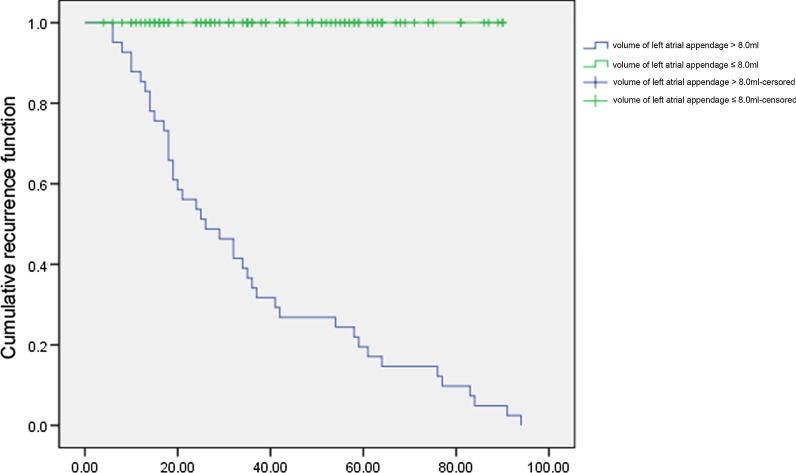
Results: According to the follow-up results, the patients were divided into two groups: the non-recurrence group and the recurrence group. P-min, PWD, P-max, PtfV1 ≥ 0.04 mV·s, PR interval prolongation, and the ratio of first and third-degree IAB in the recurrence group were higher than those in the non-recurrence group, with significant statistical differences (P < 0.05). Kaplan-Meier curve analysis was performed on time to atrial fibrillation recurrence after catheter ablation when PtfV1 ≥ 0.04 mv s by comparison between groups (Log Rank test: 2 = 4.739, P < 0.001). Kaplan-Meier curve analysis showed that the survival rate without recurrence of atrial fibrillation after catheter ablation was lower when the LLAV exceeded 8.0 mL (log-rank test P < 0.001).
Conclusion: PWD, P-max, PtfV1, PR interval prolongation, first and third-degree IAB, and LLAV can effectively predict atrial fibrillation recurrence after radiofrequency catheter ablation. The combination might be a valid and alternative independent predictor of recurrence.
Keywords: Left atrial appendage volume; P-wave ECG index; Radiofrequency catheter ablation of atrial fibrillation; Recurrence.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures





Similar articles
-
Diagnostic value of electrocardiographic P-wave characteristics in atrial fibrillation recurrence and tachycardia-induced cardiomyopathy after catheter ablation.Heart Vessels. 2018 Nov;33(11):1381-1389. doi: 10.1007/s00380-018-1179-4. Epub 2018 Apr 30. Heart Vessels. 2018. PMID: 29713820
-
Low P-wave amplitude (<0.1 mV) in lead I is associated with displaced inter-atrial conduction and clinical recurrence of paroxysmal atrial fibrillation after radiofrequency catheter ablation.Europace. 2016 Mar;18(3):384-91. doi: 10.1093/europace/euv028. Epub 2015 May 11. Europace. 2016. PMID: 25969437
-
Left atrial appendage flow velocity and time from P-wave onset to tissue Doppler-derived A' predict atrial fibrillation recurrence after radiofrequency catheter ablation.Echocardiography. 2015 Jul;32(7):1101-8. doi: 10.1111/echo.12823. Epub 2014 Nov 1. Echocardiography. 2015. PMID: 25362992
-
Prolonged P-wave duration in sinus rhythm pre-ablation is associated with atrial fibrillation recurrence after pulmonary vein isolation-A systematic review and meta-analysis.Ann Noninvasive Electrocardiol. 2019 Sep;24(5):e12653. doi: 10.1111/anec.12653. Epub 2019 Apr 14. Ann Noninvasive Electrocardiol. 2019. PMID: 30983090 Free PMC article.
-
Efficacy and safety of left atrial appendage electrical isolation during catheter ablation of atrial fibrillation: an updated meta-analysis.Europace. 2021 Feb 5;23(2):226-237. doi: 10.1093/europace/euaa266. Europace. 2021. PMID: 33324978
Cited by
-
Development and Validation of a Novel Prognostic Tool to Predict Recurrence of Paroxysmal Atrial Fibrillation after the First-Time Catheter Ablation: A Retrospective Cohort Study.Diagnostics (Basel). 2023 Mar 22;13(6):1207. doi: 10.3390/diagnostics13061207. Diagnostics (Basel). 2023. PMID: 36980515 Free PMC article.
-
Multiple anthropometric measures and proarrhythmic 12-lead ECG indices: A mendelian randomization study.PLoS Med. 2023 Aug 8;20(8):e1004275. doi: 10.1371/journal.pmed.1004275. eCollection 2023 Aug. PLoS Med. 2023. PMID: 37552661 Free PMC article.
-
Atrial Cardiomyopathy in Atrial Fibrillation: A Multimodal Diagnostic Framework.Diagnostics (Basel). 2025 May 10;15(10):1207. doi: 10.3390/diagnostics15101207. Diagnostics (Basel). 2025. PMID: 40428200 Free PMC article. Review.
-
P-wave terminal force in lead V1 is associated with recurrence after catheter ablation in patients with paroxysmal atrial fibrillation and normal left atrial size.Front Cardiovasc Med. 2024 Oct 10;11:1467585. doi: 10.3389/fcvm.2024.1467585. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39450235 Free PMC article.
-
Regional left atrial conduction velocity in the anterior wall is associated with clinical recurrence of atrial fibrillation after catheter ablation: efficacy in combination with the ipsilateral low voltage area.BMC Cardiovasc Disord. 2022 Nov 1;22(1):457. doi: 10.1186/s12872-022-02881-6. BMC Cardiovasc Disord. 2022. PMID: 36319975 Free PMC article.
References
-
- Luca F, Caretta G, Vagnarelli F, Marini M, Iorio A, Di Fusco SA, Pozzi A, GabrielliD Colivicchi F, De Luca L, et al. Clinical characteristics, management andoutcomes of patients with acute coronary syndrome and atrial fibrillation: realworlddata from two nationwide registries in Italy. J Cardiovasc Med. 2020;21(2):99–105. doi: 10.2459/JCM.0000000000000911. - DOI - PubMed
-
- Yang WY, Du X, Jiang C, He L, Fawzy AM, Wang L, Liu C, Xia SJ, Chang SS, Guo XY, et al. The safety of discontinuation of oral anticoagulation therapy after apparently successful atrial fibrillation ablation: a report from the Chinese Atrial Fibrillation Registry study. EP Europace. 2020;22(1):90–99. doi: 10.1093/europace/euz235. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
