

Left and right ventricular strain using fast strain-encoded cardiovascular magnetic resonance for the diagnostic classification of patients with chronic non-ischemic heart failure due to dilated, hypertrophic cardiomyopathy or cardiac amyloidosis
- PMID: 33823860
- PMCID: PMC8025329
- DOI: 10.1186/s12968-021-00711-w
Left and right ventricular strain using fast strain-encoded cardiovascular magnetic resonance for the diagnostic classification of patients with chronic non-ischemic heart failure due to dilated, hypertrophic cardiomyopathy or cardiac amyloidosis
Abstract
Aims: To compare the ability of left ventricular (LV) and right ventricular (RV) strain measured by fast-strain encoded cardiovascular magnetic resonance (CMR) (fast-SENC) with LV- and RV-ejection fraction for the diagnostic classification of patients with different stages of chronic heart failure (stages A-D based on American College of Cardiology/American Heart Association guidelines) due to non-ischemic cardiomyopathies.
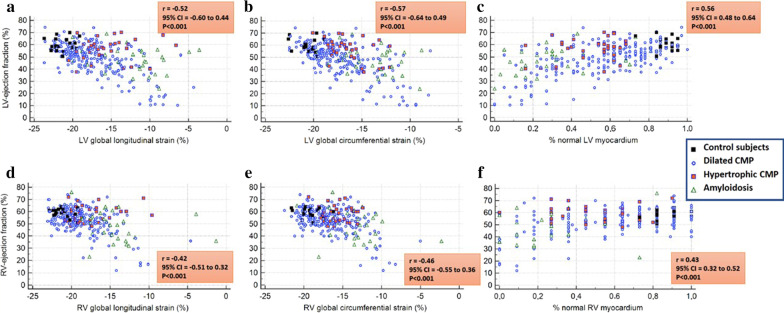
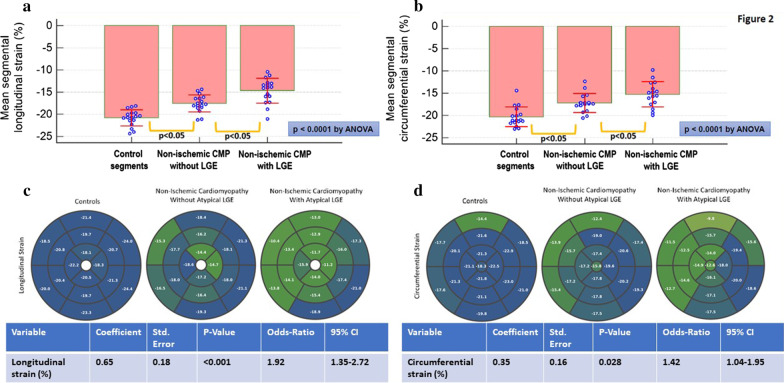
Methods: Our study population consisted of 276 consecutive patients who underwent CMR for clinical reasons, and 19 healthy subjects. Wall motion score index and non-infarct related late gadolinium enhancement (LGE), LV ejection fraction (LVEF) and RV ejection fraction (RVEF) and global LV- and RV-longitudinal (GLS) and circumferential strain (GCS) based on fast-SENC acquisitions, were calculated in all subjects. The percentage of LV and RV myocardial segments with strain ≤ - 17% (%normal LV and RV myocardium) was determined in all subjects.
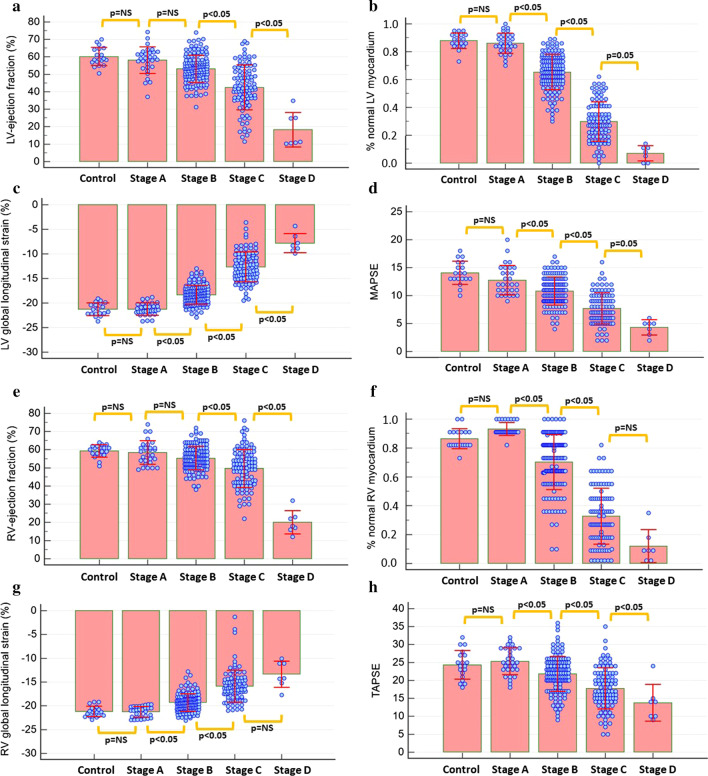
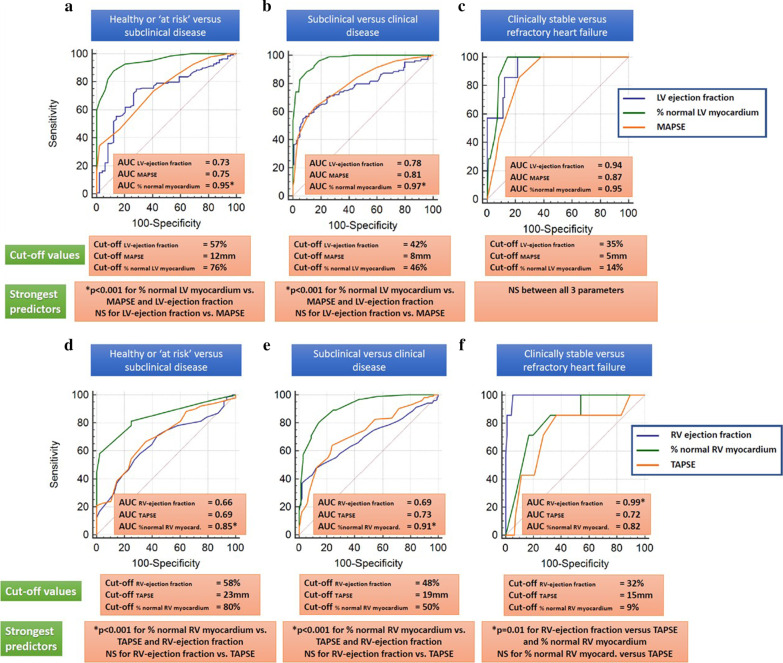
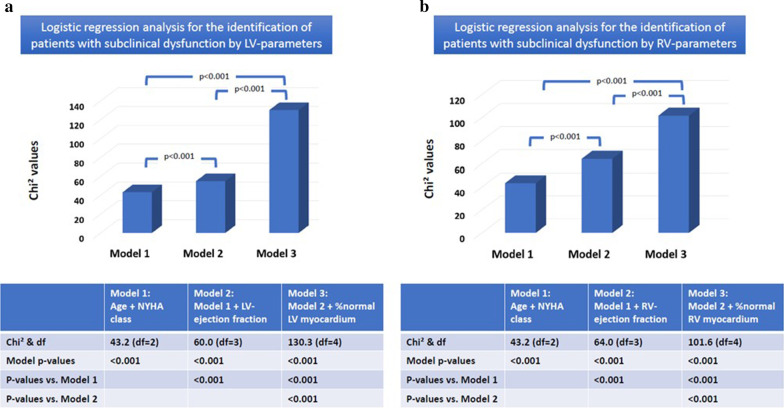
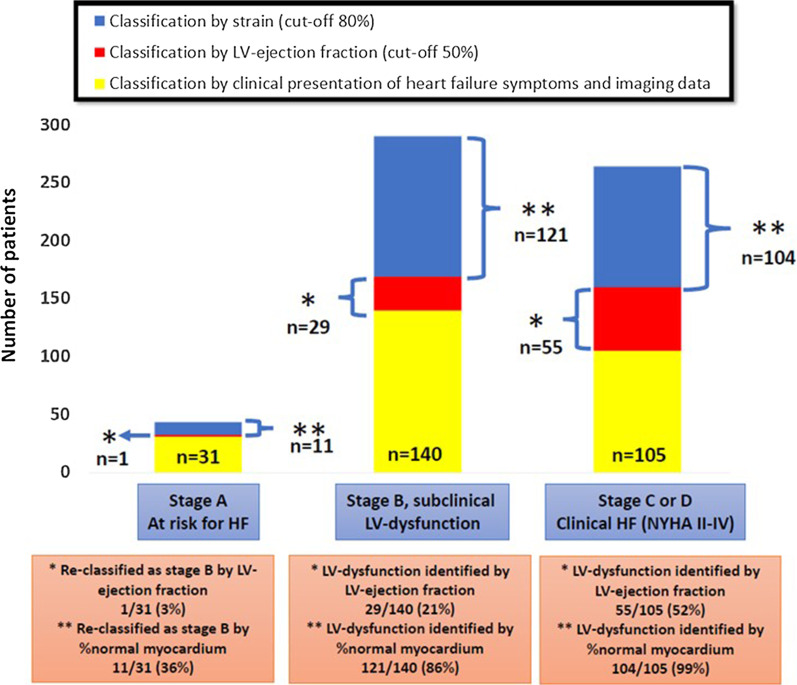
Results: LVEF and RVEF, LV-GLS, LV-GCS, RV-GLS, RV-GCS and %normal LV- and RV myocardium depressed with increasing heart failure stage (p < 0.001 for all by ANOVA). By multivariable analysis, %normal LV and RV myocardium exhibited closer associations to heart failure stages than LVEF and RVEF (rpartial = 0.79 versus rpartial = 0.21 for %normal LV myocardium versus LVEF and rpartial = 0.64 versus rpartial = 0.20 for %normal RV myocardium versus RVEF, respectively). Furthermore, %normal LV and RV myocardium exhibited incremental value for the identification of patients (i) with subclinical myocardial dysfunction and (ii) with symptomatic heart failure, surpassing that provided by LVEF and RVEF (ΔAUC = 0.22 for LVEF and ΔAUC = 0.19 for RVEF with subclinical dysfunction, and ΔAUC = 0.19 for LVEF and ΔAUC = 0.22 for RVEF with symptomatic heart failure, respectively, p < 0.001 for all). %normal LV myocardium reclassified 11 of 31 (35%) patients judged as having no structural heart disease by clinical and imaging data to stage B, i.e., subclinical LV-dysfunction.
Conclusions: In patients with non-ischemic cardiomyopathy, %normal LV and RV myocardium, by fast-SENC, enables improved identification of asymptomatic patients with subclinical LV-dysfunction. This technique may be useful for the early identification of such presumably healthy subjects at risk for heart failure and for monitoring LV and RV deformation during pharmacologic interventions in future studies.
Keywords: Cardiac magnetic resonance; Fast-strain-encoded MR (fast-SENC); Heart failure; Hypertrophy; Ischemic and non-ischemic cardiomyopathies; Late gadolinium enhancement; Myocarditis.
Conflict of interest statement
H.S. and S.K. received research Grants from Myocardial Solutions. S.K. owns stock options of Myocardial Solutions. All other authors declare that they have no competing interests regarding this manuscript.
Figures
Similar articles
-
Fast Strain-Encoded Cardiac Magnetic Resonance for Diagnostic Classification and Risk Stratification of Heart Failure Patients.JACC Cardiovasc Imaging. 2021 Jun;14(6):1177-1188. doi: 10.1016/j.jcmg.2020.10.024. Epub 2021 Jan 13. JACC Cardiovasc Imaging. 2021. PMID: 33454266
-
Right ventricular function declines prior to left ventricular ejection fraction in hypertrophic cardiomyopathy.J Cardiovasc Magn Reson. 2022 Jun 13;24(1):36. doi: 10.1186/s12968-022-00868-y. J Cardiovasc Magn Reson. 2022. PMID: 35692049 Free PMC article.
-
Prognostic value of myocardial strain and late gadolinium enhancement on cardiovascular magnetic resonance imaging in patients with idiopathic dilated cardiomyopathy with moderate to severely reduced ejection fraction.J Cardiovasc Magn Reson. 2018 Jun 14;20(1):36. doi: 10.1186/s12968-018-0466-7. J Cardiovasc Magn Reson. 2018. PMID: 29898740 Free PMC article.
-
Myocardial Strain Measurements Derived From MR Feature-Tracking: Influence of Sex, Age, Field Strength, and Vendor.JACC Cardiovasc Imaging. 2024 Apr;17(4):364-379. doi: 10.1016/j.jcmg.2023.05.019. Epub 2023 Jul 19. JACC Cardiovasc Imaging. 2024. PMID: 37480906
-
Effect of Chronic Obstructive Pulmonary Disease (COPD) on Biventricular Mechanics in Patients Without Severe Airflow Obstruction.J Clin Med. 2025 May 23;14(11):3660. doi: 10.3390/jcm14113660. J Clin Med. 2025. PMID: 40507423 Free PMC article. Review.
Cited by
-
Prognostic Value of Cardiac Magnetic Resonance in Assessing Right Ventricular Strain in Cardiovascular Disease: A Systematic Review and Meta-Analysis.Rev Cardiovasc Med. 2022 Dec 12;23(12):406. doi: 10.31083/j.rcm2312406. eCollection 2022 Dec. Rev Cardiovasc Med. 2022. PMID: 39076664 Free PMC article.
-
Multi-parametric assessment of left ventricular hypertrophy using late gadolinium enhancement, T1 mapping and strain-encoded cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2021 Jul 12;23(1):92. doi: 10.1186/s12968-021-00775-8. J Cardiovasc Magn Reson. 2021. PMID: 34247623 Free PMC article.
-
Clinical and Cardiovascular Magnetic Resonance Imaging Features of Cardiac Amyloidosis.Rev Cardiovasc Med. 2023 Oct 16;24(10):291. doi: 10.31083/j.rcm2410291. eCollection 2023 Oct. Rev Cardiovasc Med. 2023. PMID: 39077571 Free PMC article. Review.
-
CMR-based right ventricular strain analysis in cardiac amyloidosis and its potential as a supportive diagnostic feature.Int J Cardiol Heart Vasc. 2022 Dec 28;44:101167. doi: 10.1016/j.ijcha.2022.101167. eCollection 2023 Feb. Int J Cardiol Heart Vasc. 2022. PMID: 36632287 Free PMC article.
-
Examining the Difficulties in Identifying and Handling Cardiac Amyloidosis; Acquiring Important Knowledge and Robust Treatment Methods.Cardiovasc Hematol Disord Drug Targets. 2024;24(2):65-82. doi: 10.2174/011871529X301954240715041558. Cardiovasc Hematol Disord Drug Targets. 2024. PMID: 39075963 Review.
References
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113(14):1807–1816. doi: 10.1161/CIRCULATIONAHA.106.174287. - DOI - PubMed
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29(2):270–276. doi: 10.1093/eurheartj/ehm342. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
