

T cell assays differentiate clinical and subclinical SARS-CoV-2 infections from cross-reactive antiviral responses
- PMID: 33824342
- PMCID: PMC8024333
- DOI: 10.1038/s41467-021-21856-3
T cell assays differentiate clinical and subclinical SARS-CoV-2 infections from cross-reactive antiviral responses
Abstract
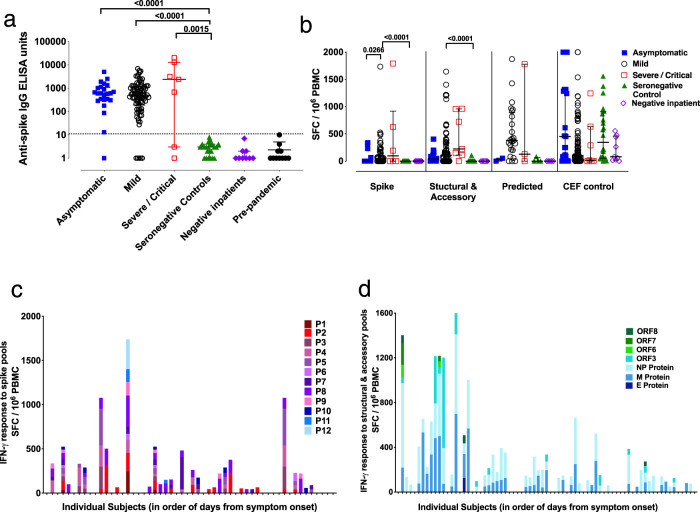
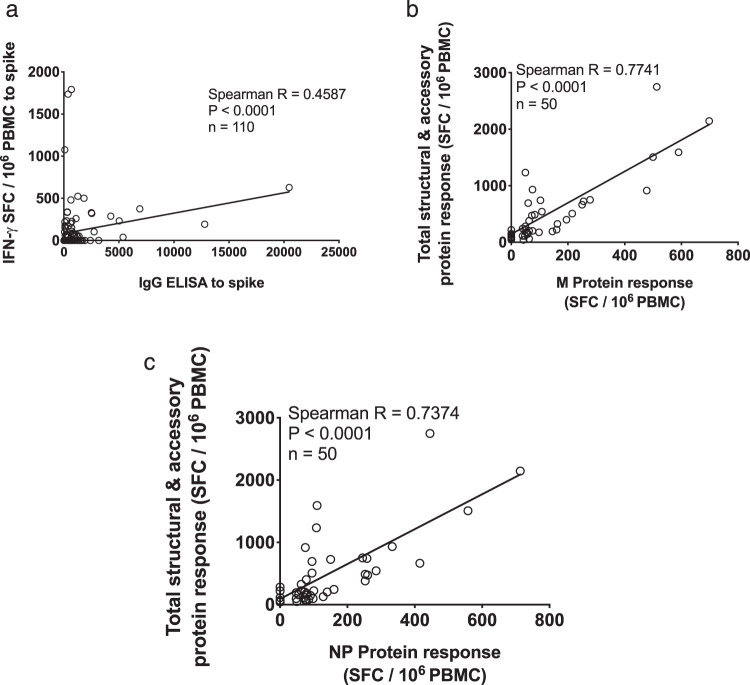
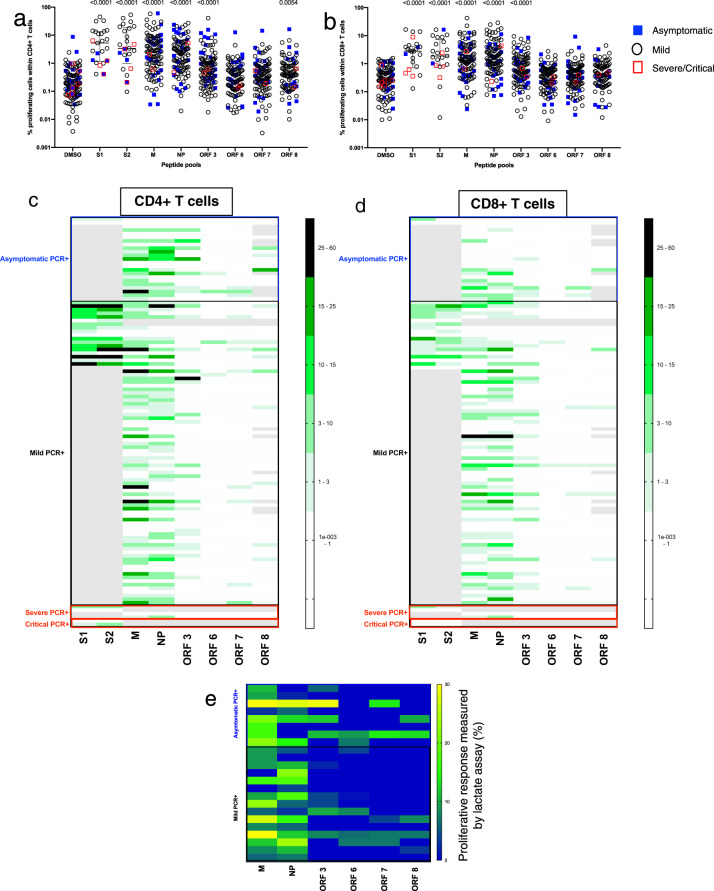
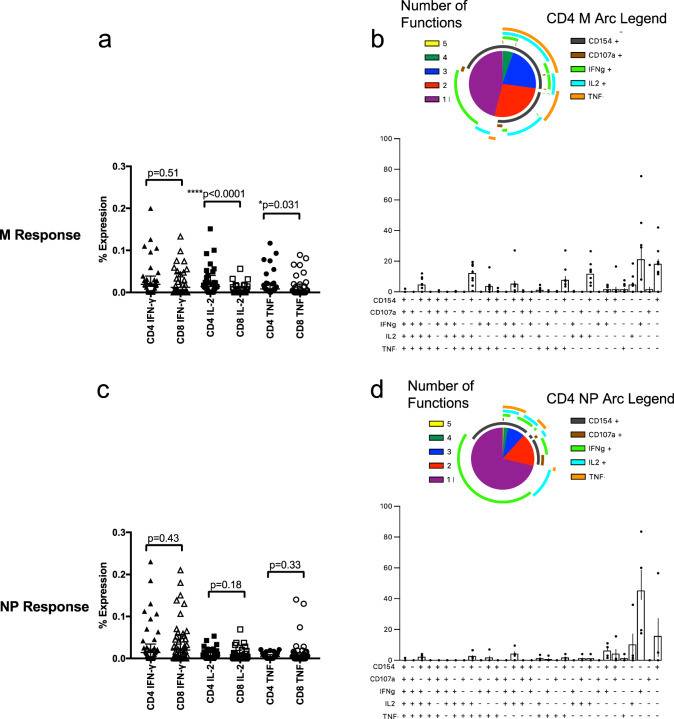
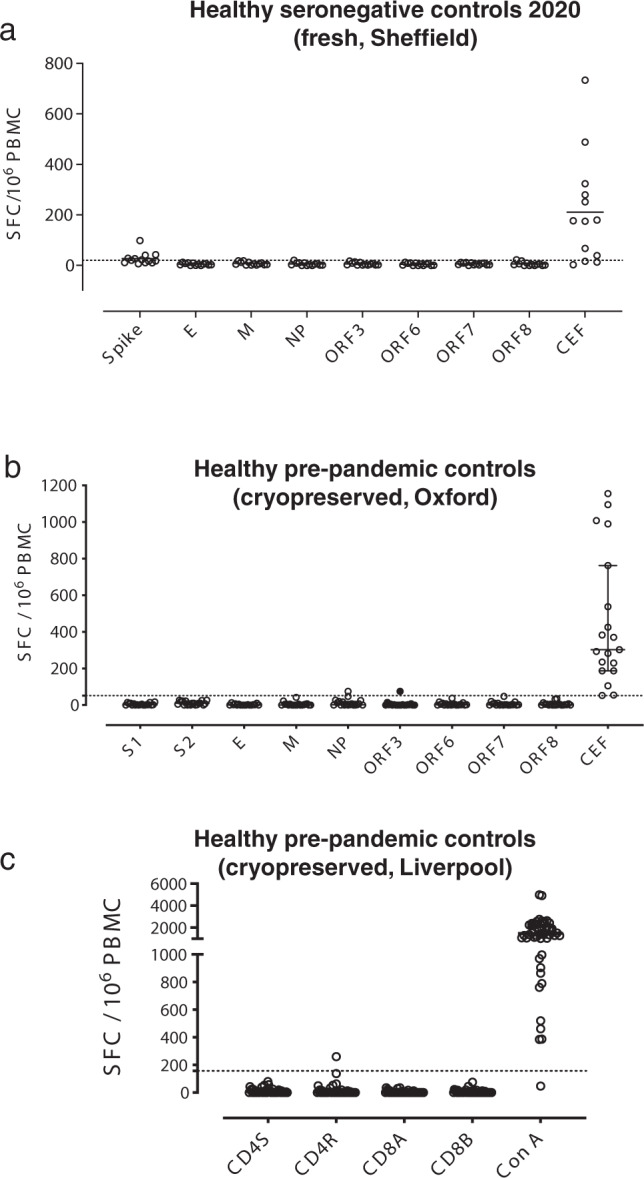
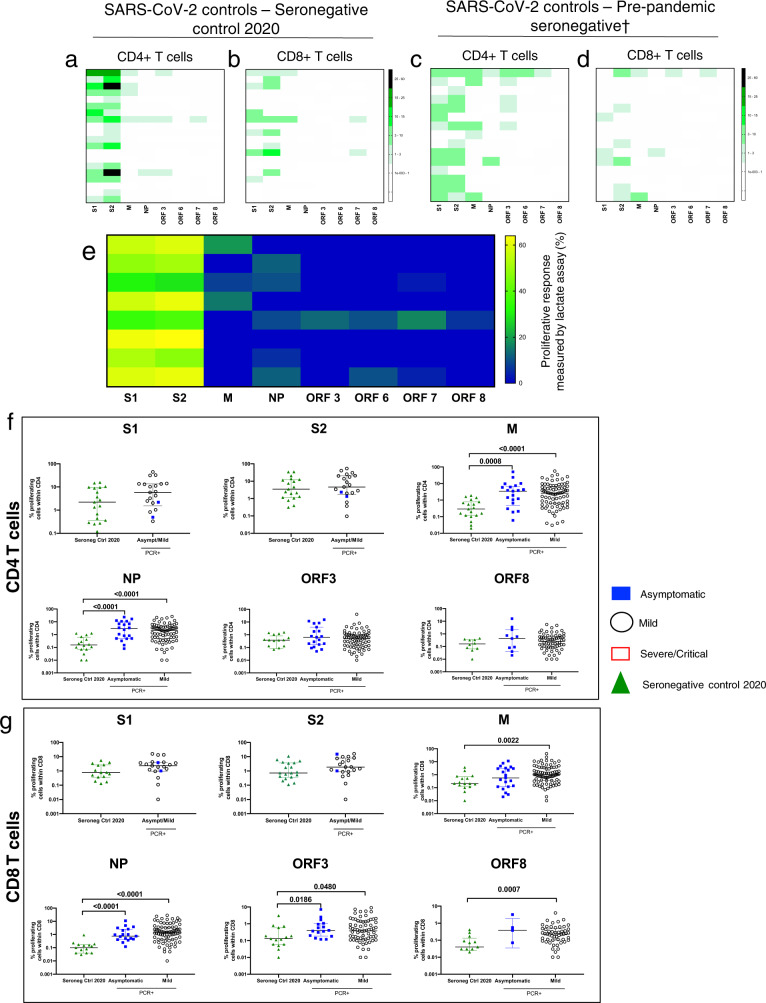
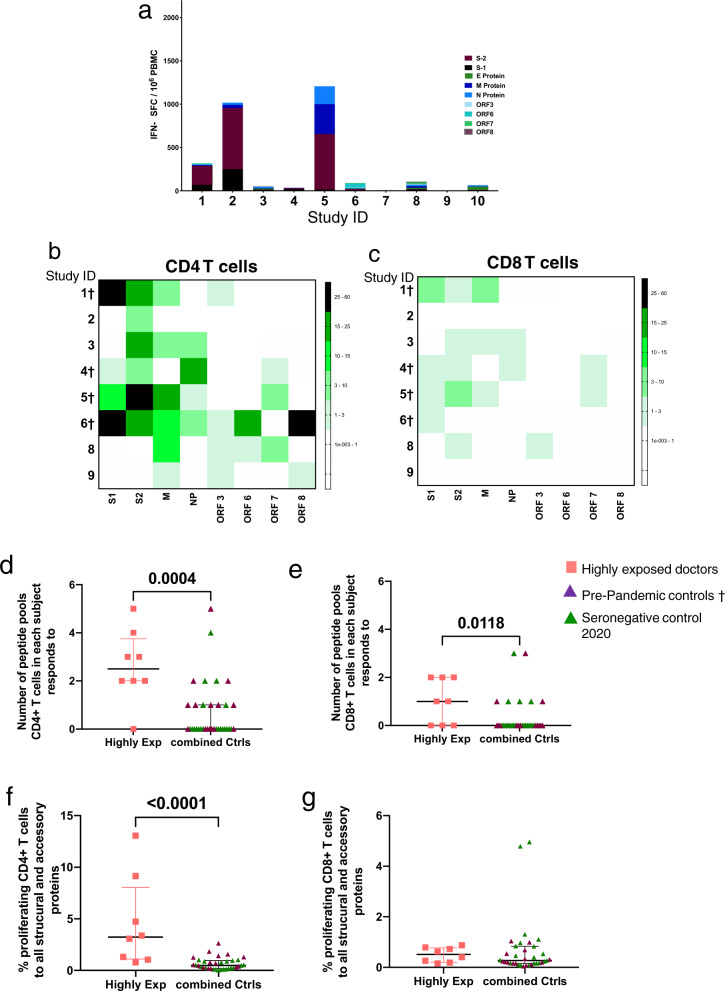
Identification of protective T cell responses against SARS-CoV-2 requires distinguishing people infected with SARS-CoV-2 from those with cross-reactive immunity to other coronaviruses. Here we show a range of T cell assays that differentially capture immune function to characterise SARS-CoV-2 responses. Strong ex vivo ELISpot and proliferation responses to multiple antigens (including M, NP and ORF3) are found in 168 PCR-confirmed SARS-CoV-2 infected volunteers, but are rare in 119 uninfected volunteers. Highly exposed seronegative healthcare workers with recent COVID-19-compatible illness show T cell response patterns characteristic of infection. By contrast, >90% of convalescent or unexposed people show proliferation and cellular lactate responses to spike subunits S1/S2, indicating pre-existing cross-reactive T cell populations. The detection of T cell responses to SARS-CoV-2 is therefore critically dependent on assay and antigen selection. Memory responses to specific non-spike proteins provide a method to distinguish recent infection from pre-existing immunity in exposed populations.
Conflict of interest statement
D.W.E. declares lecture fees from Gilead. A.S. is listed as an inventor on patent application no. 63/012,902, submitted by La Jolla Institute for Immunology, covers the use of the megapools and peptides thereof for therapeutic and diagnostic purposes. A.S. is a consultant for Gritstone and Flow Pharma and Avalia. The remaining authors declare no competing interests.
Figures
References
-
- Gorbalenya AE, et al. Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020;5:536–544. doi: 10.1038/s41564-020-0695-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_PC_19059/MRC_/Medical Research Council/United Kingdom
- 110110/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MC_PC_20002/MRC_/Medical Research Council/United Kingdom
- MR/V028448/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00008/5/MRC_/Medical Research Council/United Kingdom
- MR/L006758/1/MRC_/Medical Research Council/United Kingdom
- 108869/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MR/L006588/1/MRC_/Medical Research Council/United Kingdom
- NIHR200907/DH_/Department of Health/United Kingdom
- 205228/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 220171/Z/20/Z/WT_/Wellcome Trust/United Kingdom
- MR/P011233/1/MRC_/Medical Research Council/United Kingdom
- 109965/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MR/L018942/1/MRC_/Medical Research Council/United Kingdom
- WT109965MA/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
