

Epidemiologic trends of infants with orofacial clefts in a multiethnic country: a retrospective population-based study
- PMID: 33824370
- PMCID: PMC8024282
- DOI: 10.1038/s41598-021-87229-4
Epidemiologic trends of infants with orofacial clefts in a multiethnic country: a retrospective population-based study
Abstract
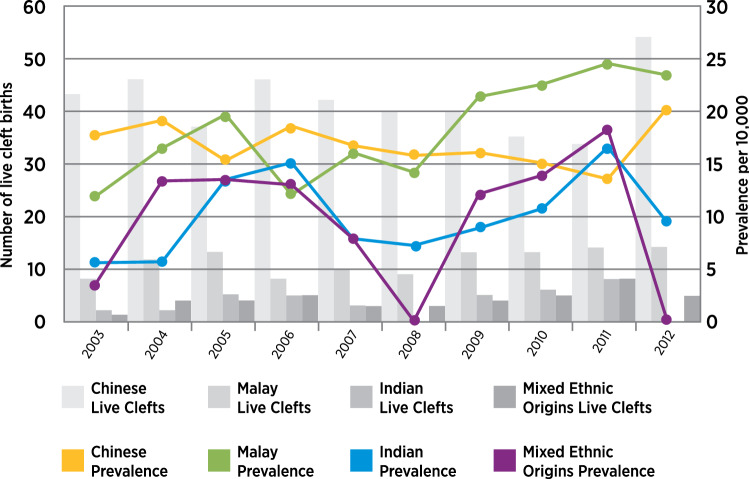
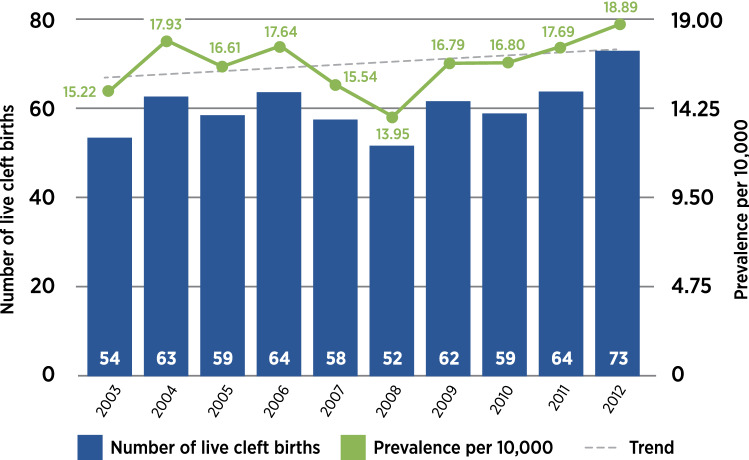
Cleft births surveillance is essential in healthcare and prevention planning. Data are needed in precision medicine to target upstream management for at-risk individuals. This study characterizes Singapore's population-based orofacial cleft topography by ethnicity and gender, and establishes the cleft cohort's infant mortality rate. Data, in the decade 2003 to 2012, were extracted by the National Birth Defects Registry. Trend testing by linear regression was at p < 0.05 significance level. Prevalence per 10,000 for population-based cleft live births was 16.72 with no significant upward trend (p = 0.317). Prevalence rates were 8.77 in the isolated cleft group, 7.04 in the non-isolated cleft group, and 0.91 in the syndromic cleft group. There was significant upward trend in infants with non-isolated clefts (p = 0.0287). There were no significant upward trends in infants with isolated clefts and syndromic clefts. Prevalence rates were sexually dimorphic and ethnic-specific: male 17.72; female 15.78; Chinese group 17.17; Malay group 16.92; Indian group 10.74; and mixed ethnic origins group 21.73. The overall infant mortality rate (IMR) was 4.8% in the cohort of 608 cleft births, which was more than double the population-based IMR of 2.1% in the same period. Infants with non-isolated and syndromic clefts accounted for 96.6% of the deaths.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Fogh-Andersen P. Inheritance of Harelip and Cleft Palate. Nyt Nordisk Forlag; 1942.
-
- Jensen BL, Kreiborg S, Dahl E, Fogh-Andersen P. Cleft lip and palate in Denmark, 1976–1981: Epidemiology, variability, and early somatic development. Cleft Palate J. 1988;25:258–269. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
