

Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19
- PMID: 33824483
- PMCID: PMC8023349
- DOI: 10.1038/s41577-021-00536-9
Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19
Abstract
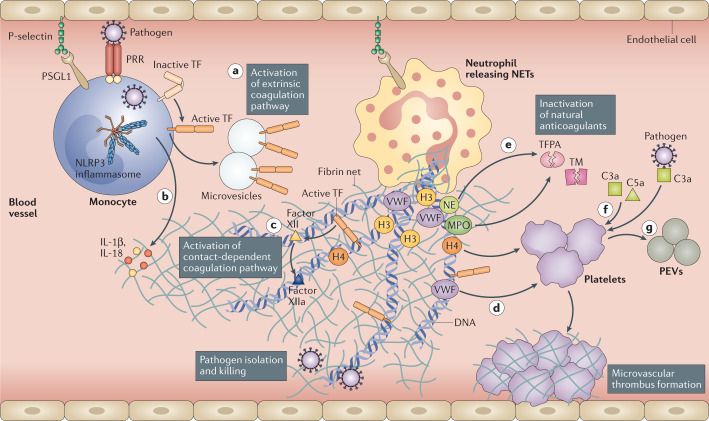
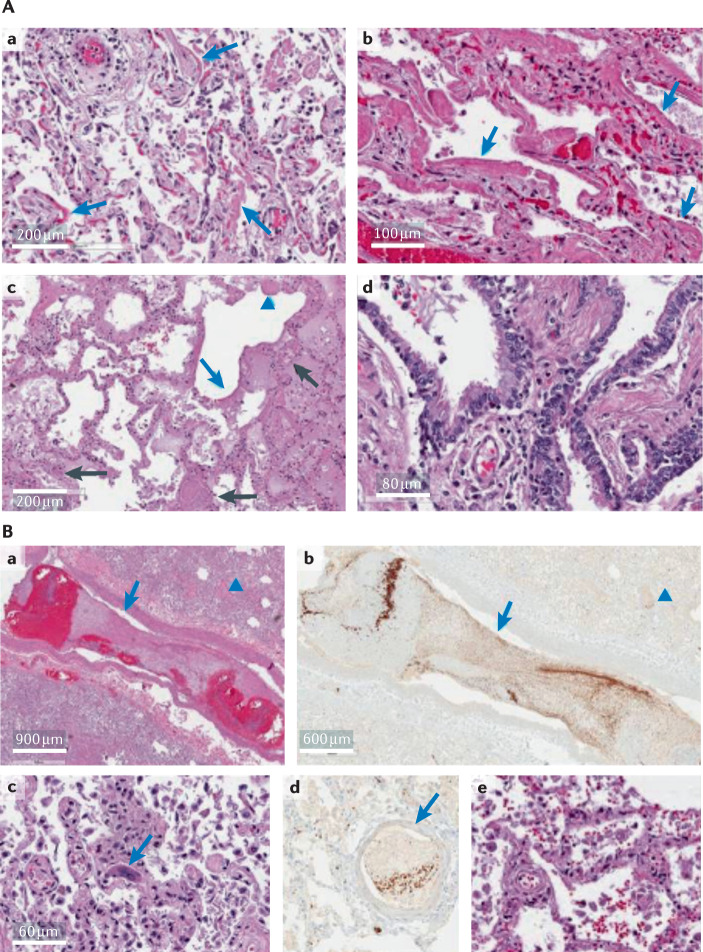
Coronavirus disease 2019 (COVID-19) is a clinical syndrome caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Patients with severe disease show hyperactivation of the immune system, which can affect multiple organs besides the lungs. Here, we propose that SARS-CoV-2 infection induces a process known as immunothrombosis, in which activated neutrophils and monocytes interact with platelets and the coagulation cascade, leading to intravascular clot formation in small and larger vessels. Microthrombotic complications may contribute to acute respiratory distress syndrome (ARDS) and other organ dysfunctions. Therapeutic strategies aimed at reducing immunothrombosis may therefore be useful. Several antithrombotic and immunomodulating drugs have been proposed as candidates to treat patients with SARS-CoV-2 infection. The growing understanding of SARS-CoV-2 infection pathogenesis and how it contributes to critical illness and its complications may help to improve risk stratification and develop targeted therapies to reduce the acute and long-term consequences of this disease.
Conflict of interest statement
A.B. and A.V. received a travel grant from Kiniksa Pharmaceuticals Ltd and honoraria from Effetti s.r.l. (Milan, Italy). L.D. has received consultation honoraria from Abbvie, Amgen, Biogen, Bristol-Myers Squibb, Celltrion, GlaxoSmithKline, Novartis, Pfizer, Roche, Sanofi-Genzyme and SOBI. K.M. is an inventor on patent US9642822 and patent applications WO20180271953A1 and US2019167680A1, and is a consultant for PEEL Therapeutics, Inc. B.W.V.T. has served as a consultant for Novartis and Serpin Pharma, and has received research support from Novartis, Kiniksa Pharmaceuticals Ltd, Serpin Pharma and SOBI. A.A. has served as a consultant for Applied Clinical Intel, AstraZeneca, Cromos Pharma, Janssen, Kiniksa Pharmaceuticals Ltd, Merck, Olatec and Serpin Pharma, and has received research support from Janssen, Olatec and Serpin Pharma. All other authors declare no competing interests.
Figures
Comment in
-
Oxygen-ozone treatment and COVID-19: antioxidants targeting endothelia lead the scenery.Intern Emerg Med. 2022 Mar;17(2):593-596. doi: 10.1007/s11739-021-02865-y. Epub 2021 Oct 22. Intern Emerg Med. 2022. PMID: 34677789 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
