

Craniovertebral junction instability in Larsen syndrome: An institutional series and review of literature
- PMID: 33824557
- PMCID: PMC8019120
- DOI: 10.4103/jcvjs.JCVJS_164_20
Craniovertebral junction instability in Larsen syndrome: An institutional series and review of literature
Abstract
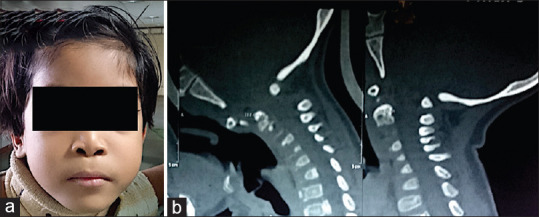
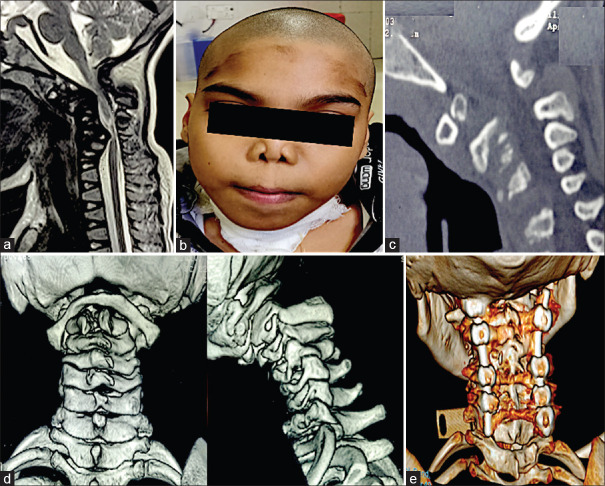
Objective: Larsen syndrome (LS) is characterized by osteo-chondrodysplasia, multiple joint dislocations, and craniofacial abnormalities. Symptomatic myelopathy is attributed to C1-C2 instability and sub-axial cervical kyphosis. In this article, we have analyzed the surgical outcome after posterior fixation in LS with craniovertebral junction instability.
Methods: Ten symptomatic pediatric patients, operated between 2011 and 2019, were included, and the clinical outcome was assessed by Nurick grade, neurological improvement, and complications. The requirement of anti-spasticity drugs, the degree of bony fusion, and restriction of neck movement were also noted. At last follow-up, patient satisfaction score (PSS) and back to school status were studied. We also reviewed the literature and categorized two types of presentation of reported LS patients and discussed the pattern of disease progression among both.
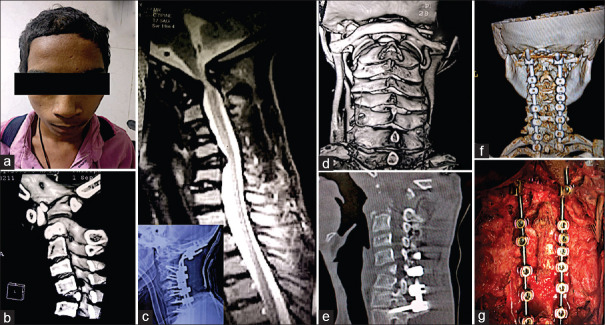
Results: Ten patients, age range 1.5-16 years, underwent 12 surgeries (6 C1-C2 fixation, 4 long-segment posterior cervical fixation, and 2 trans-oral decompressions as the second stage); the mean follow-up was 23 (range, 6-86 months). All the ten patients in our study had the characteristic "dish-" like face and nine patients had acral anomalies. The median Nurick grade improved from preoperative (median = 4) to follow-up (median = 3). The requirement of anti-spasticity drugs decreased in seven patients and the neck-pain improved in nine patients. The median satisfaction at follow-up was good (median PSS = 2); five patients were going back to school.
Conclusion: Craniovertebral junction instability in LS is rare and surgically challenging. Early posterior fixation showed a promising outcome with a halt in the disease progression.
Keywords: Cervical kyphosis; Larsen syndrome; cranio-vertebral junction anomalies; long segment fusion; sub-axial compression; syndromic atlantoaxial dislocation.
Copyright: © 2020 Journal of Craniovertebral Junction and Spine.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Retro-odontoid Degenerative Pseudotumour Causing Spinal Cord Compression and Myelopathy: Current Evidence on the Role of Posterior C1-C2 Fixation in Treatment.Acta Neurochir Suppl. 2019;125:259-264. doi: 10.1007/978-3-319-62515-7_37. Acta Neurochir Suppl. 2019. PMID: 30610331 Review.
-
Fusions at the craniovertebral junction.Childs Nerv Syst. 2008 Oct;24(10):1209-24. doi: 10.1007/s00381-008-0607-7. Epub 2008 Apr 4. Childs Nerv Syst. 2008. PMID: 18389260 Review.
-
C1-C2 transarticular screw fixation for atlantoaxial instability due to rheumatoid arthritis: a seven-year analysis of outcome.Spine (Phila Pa 1976). 2009 Dec 15;34(26):2880-5. doi: 10.1097/BRS.0b013e3181b4e218. Spine (Phila Pa 1976). 2009. PMID: 20010395
-
Outcome of Surgery for Congenital Craniovertebral Junction Anomalies with Atlantoaxial Dislocation/Basilar Invagination: A Retrospective Study of 94 Patients.World Neurosurg. 2021 Feb;146:e313-e322. doi: 10.1016/j.wneu.2020.10.082. Epub 2020 Oct 20. World Neurosurg. 2021. PMID: 33096283
-
Larsen syndrome with C3-C4 spondyloptosis and atlantoaxial dislocation in an adult.Spine (Phila Pa 1976). 2013 Jan 1;38(1):E43-7. doi: 10.1097/BRS.0b013e318278e59d. Spine (Phila Pa 1976). 2013. PMID: 23080426
Cited by
-
Larsen Syndrome and Associated Spinal Deformities.Cureus. 2023 Jul 10;15(7):e41655. doi: 10.7759/cureus.41655. eCollection 2023 Jul. Cureus. 2023. PMID: 37565102 Free PMC article. Review.
References
-
- Menezes AH. Craniovertebral junction database analysis: Incidence, classification, presentation, and treatment algorithms. Childs Nerv Syst. 2008;24:1101–8. - PubMed
-
- Sardhara J, Behari S, Jaiswal AK, Srivastava A, Sahu RN, Mehrotra A, et al. Syndromic versus nonsyndromic atlantoaxial dislocation: Do clinical-radiological differences have a bearing on management? Acta Neurochir (Wien) 2013;155:1157–67. - PubMed
-
- Sakaura H, Matsuoka T, Iwasaki M, Yonenobu K, Yoshikawa H. Surgical treatment of cervical kyphosis in Larsen syndrome: Report of 3 cases and review of the literature. Spine (Phila Pa 1976) 2007;32:E39–44. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous