Diffuse cutaneous mastocytosis masquerading as linear IgA bullous dermatosis of childhood
- PMID: 33824710
- PMCID: PMC8018259
- DOI: 10.4081/dr.2021.9021
Diffuse cutaneous mastocytosis masquerading as linear IgA bullous dermatosis of childhood
Abstract
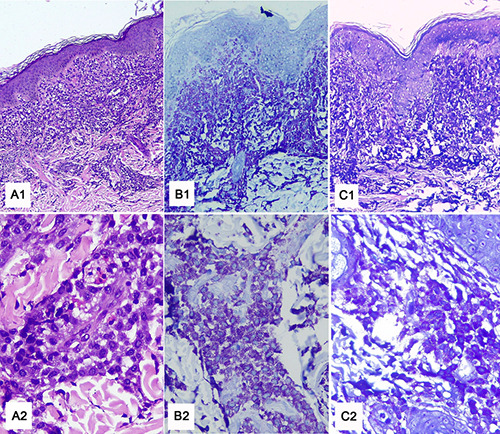
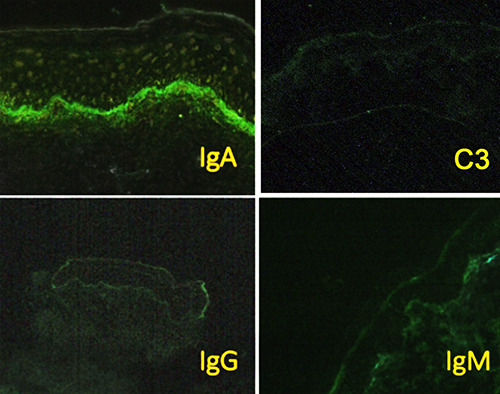
Diffuse cutaneous mastocytosis is a rare form of cutaneous mastocytosis that can appear in heterogeneous clinical presentations, including eruption of papules, erythematous plaques, blisters, and erythroderma. We report a 1.5- year-old boy who presented with itchy wheals and blisters spreading on his body. The patient was initially managed as a linear IgA bullous dermatosis of childhood (LABD) because of the similarity of clinical symptoms and the presenting of linear IgA deposits at the basement membrane. Due to the development of urticarial plaque after the resolution of the blisters, the diagnosis of diffuse cutaneous mastocytosis was made based on clinical, histopathological (hematoxylin-eosin, Giemsa, and toluidine blue staining), and direct immunofluorescent examinations (IgA, IgG, IgM, C3). The symptoms were improved following antihistamines and oral corticosteroid treatment.
Keywords: Cutaneous mastocytosis; bullous mastocytosis; chronic bullous disease of childhood; linear IgA dermatosis of childhood.
©Copyright: the Author(s).
Conflict of interest statement
Conflict of interest: The authors declare no potential conflict of interest.
Figures

Similar articles
-
Unusual clinicopathological and immunological presentation of chronic bullous dermatosis of childhood (linear IgA dermatosis).Indian J Dermatol. 2011 Sep-Oct;56(5):573-5. doi: 10.4103/0019-5154.87159. Indian J Dermatol. 2011. PMID: 22121282 Free PMC article.
-
Bullous Pemphigoid Masquerading as Erythema Annulare Centrifugum.Acta Dermatovenerol Croat. 2017 Oct;25(3):255-256. Acta Dermatovenerol Croat. 2017. PMID: 29252183
-
Linear IgA bullous dermatosis of childhood.Dermatol Online J. 2022 Oct 15;28(5). doi: 10.5070/D328559270. Dermatol Online J. 2022. PMID: 36809139
-
Urticarial Lesions in a Pregnant Woman.Acta Dermatovenerol Croat. 2018 Apr;26(1):71-72. Acta Dermatovenerol Croat. 2018. PMID: 29782306 Review.
-
Linear IgA bullous dermatosis associated with ulcerative colitis: A case report and literature review.Australas J Dermatol. 2020 Feb;61(1):e82-e86. doi: 10.1111/ajd.13121. Epub 2019 Jul 18. Australas J Dermatol. 2020. PMID: 31319433 Review.
Cited by
-
Diffuse Cutaneous Mastocytosis: A Current Understanding of a Rare Disease.Int J Mol Sci. 2024 Jan 23;25(3):1401. doi: 10.3390/ijms25031401. Int J Mol Sci. 2024. PMID: 38338679 Free PMC article. Review.
-
Current Challenges in the Diagnosis of Pediatric Cutaneous Mastocytosis.Diagnostics (Basel). 2023 Dec 1;13(23):3583. doi: 10.3390/diagnostics13233583. Diagnostics (Basel). 2023. PMID: 38066824 Free PMC article. Review.
-
Repositioning Drugs for Rare Diseases Based on Biological Features and Computational Approaches.Healthcare (Basel). 2022 Sep 16;10(9):1784. doi: 10.3390/healthcare10091784. Healthcare (Basel). 2022. PMID: 36141396 Free PMC article.
References
-
- Ben-Amitai D, Metzker A, Cohen HA. Pediatric cutaneous mastocytosis : a review of 180 Patients. Isr Med Assoc J 2005;7:320-2. - PubMed
-
- Nettleship E. Rare form of urticaria. Br Med J 1869;2:323–4.
-
- Brockow K. Epidemiology, prognosis, and risk factors in mastocytosis. Immunol Allergy Clin North Am 2014;34:283–95. - PubMed
-
- Méni C, Bruneau J, Georgin-Lavialle S, et al. . Paediatric mastocytosis: a systematic review of 1747 cases. Br J Dermatol 2015;172:642–51. - PubMed
-
- Neri I, Guareschi E, Guerrini V, Patrizi A. Familial teleangiectasia macularis eruptiva perstans. Pediatr Dermatol 2005;22:488–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous