

From Neck Pain to Sarcoidosis: The Interesting Association
- PMID: 33824771
- PMCID: PMC7985240
- DOI: 10.1155/2021/6663519
From Neck Pain to Sarcoidosis: The Interesting Association
Abstract
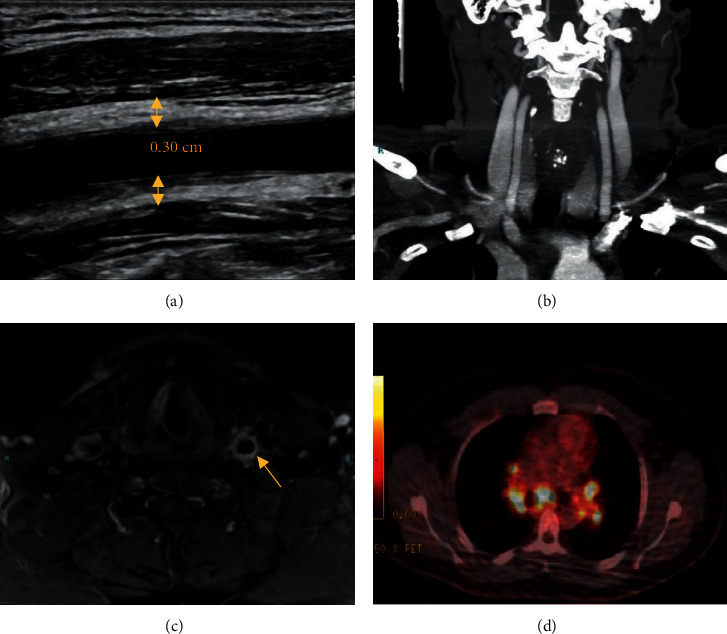
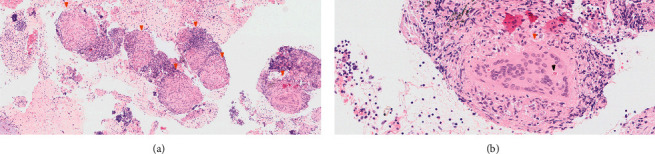
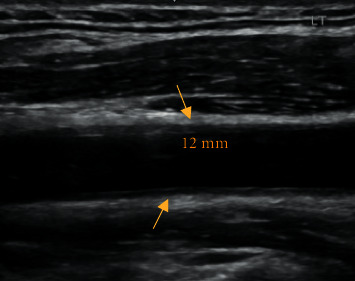
We report the case of a 31-year-old male patient, presenting to the emergency department (ED) with a 6-week history of left-sided lateral neck pain, along with a minor localized swelling. A few weeks after the beginning of his complaints, he contracted a mild coronavirus disease 2019 (COVID-19). Upon examination, his aches were defined as carotidynia; thus, proper radiologic evaluation was carried out. While ultrasound (US) and magnetic resonance imaging (MRI) scans showed evident signs of left common carotid (LCC) vasculitis, computed tomography angiography (CTA) and positron emission tomography-CT (PET-CT) scans revealed no vascular findings. Unexpected hypermetabolic hilar and mediastinal lymphadenopathy was found on PET-CT, necessitating lymph node biopsy. Pathology results displayed noncaseating granulomas. Besides, angiotensin-converting enzyme (ACE) levels in blood were high. Sarcoidosis, with concurrent LCC vasculitis, was diagnosed, and corticosteroid therapy was started. Shortly thereafter, remarkable recovery ensued.
Copyright © 2021 Fadi Kharouf et al.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Villa-Forte, Hoffman G. Systemic vasculitis in sarcoidosis. In: Hoffman G. S., Weyand C. M., Langford C. A., Goronzy J. J., editors. Inflammatory Diseases of Blood Vessels. 2nd. Hoboken, NJ, USA: Blackwell Publishing Ltd; 2012. pp. 451–459. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
