

Effects of SlowMo, a Blended Digital Therapy Targeting Reasoning, on Paranoia Among People With Psychosis: A Randomized Clinical Trial
- PMID: 33825827
- PMCID: PMC8027943
- DOI: 10.1001/jamapsychiatry.2021.0326
Effects of SlowMo, a Blended Digital Therapy Targeting Reasoning, on Paranoia Among People With Psychosis: A Randomized Clinical Trial
Abstract
Importance: Persistent paranoia is common among patients with psychosis. Cognitive-behavioral therapy for psychosis can be effective. However, challenges in engagement and effectiveness remain.
Objective: To investigate the effects on paranoia and mechanisms of action of SlowMo, a digitally supported reasoning intervention, plus usual care compared with usual care only.
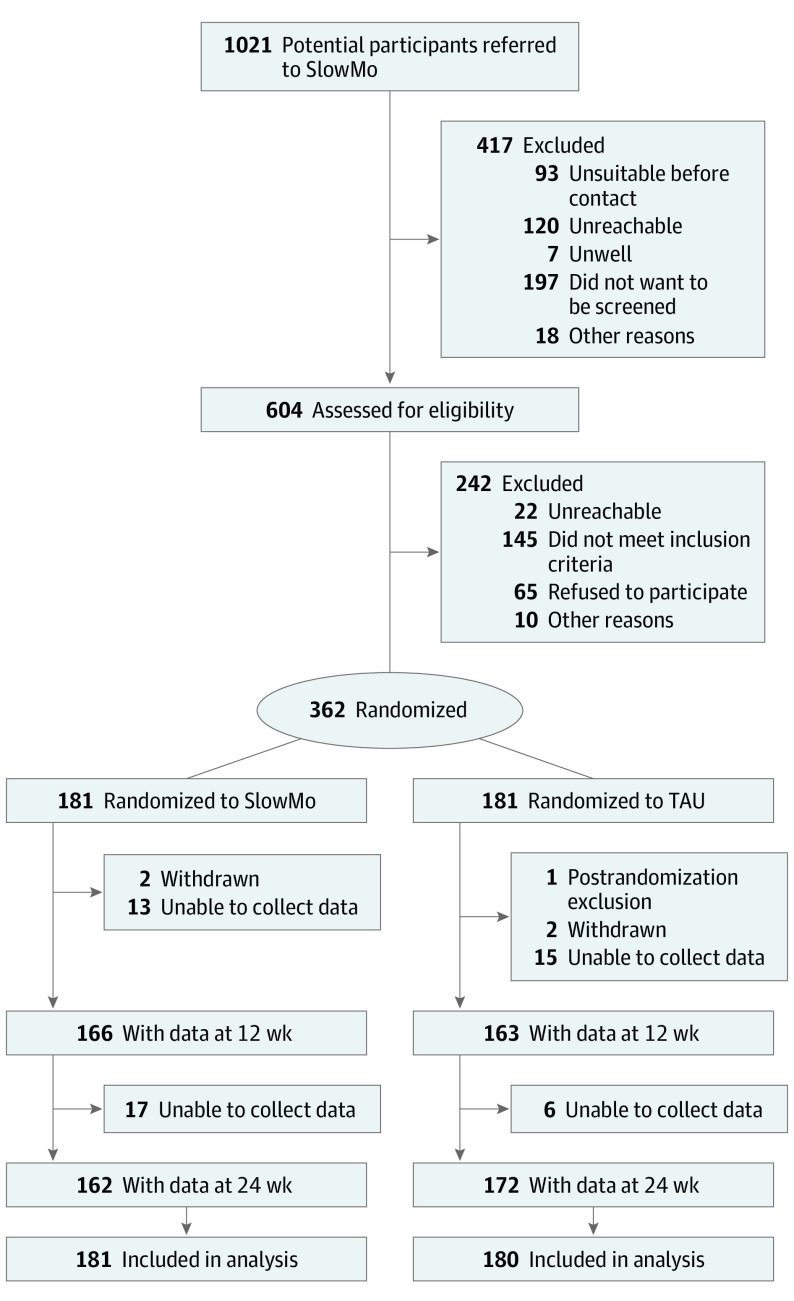
Design, setting, and participants: This parallel-arm, assessor-blinded, randomized clinical trial recruited participants at UK community health services from May 1, 2017, to May 14, 2019. Eligible participants consisted of a referral sample with schizophrenia-spectrum psychosis and distressing, persistent (≥3 months) paranoia.
Interventions: Individuals were randomized 1:1 to SlowMo, consisting of 8 digitally supported face-to-face sessions and a mobile app, plus usual care (n = 181) and usual care only (n = 181).
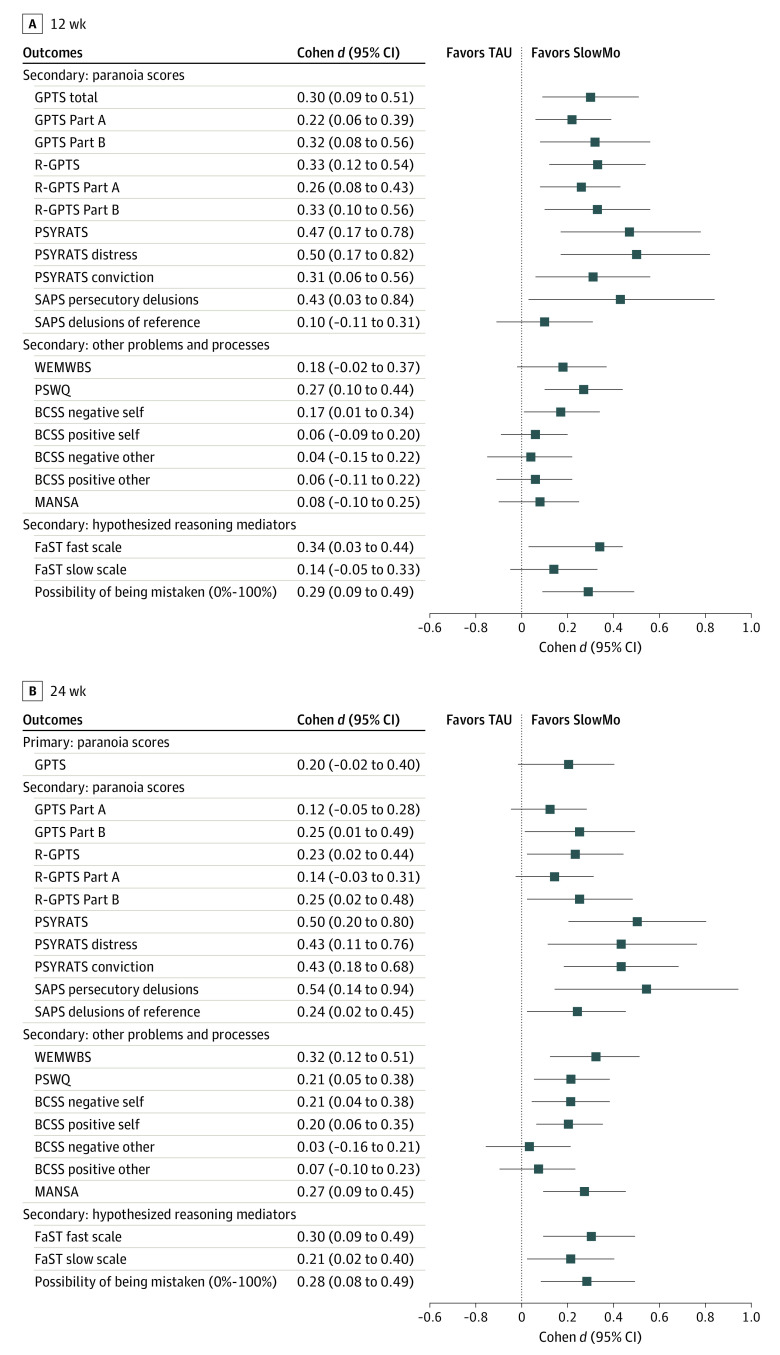
Main outcomes and measures: The primary outcome was paranoia, measured by the Green et al Paranoid Thoughts Scale (GPTS) total score at 24 weeks. Secondary outcomes included GPTS total score at 12 weeks and GPTS Part A (reference) and Part B (persecutory) scores, the Psychotic Symptom Rating Scales (PSYRATS Delusion subscale), reasoning (belief flexibility, possibility of being mistaken [Maudsley Assessment of Delusions, rated 0%-100%]), and jumping to conclusions (Beads Task).
Results: A total of 361 participants were included in intention-to-treat analysis, of whom 252 (69.8%) were male and 249 (69.0%) were White; the mean (SD) age was 42.6 (11.6) years. At 24 weeks, 332 participants (92.0%) provided primary outcome data. Of 181 participants in the SlowMo group, 145 (80.1%) completed therapy. SlowMo plus usual care was not associated with greater reductions than usual care in GPTS total score at 24 weeks (Cohen d, 0.20; 95% CI, -0.02 to 0.40; P = .06). There were significant effects on secondary paranoia outcomes at 12 weeks, including GPTS total score (Cohen d, 0.30; 95% CI, 0.09-0.51; P = .005), Part A score (Cohen d, 0.22; 95% CI, 0.06-0.39; P = .009), and Part B score (Cohen d, 0.32; 95% CI, 0.08-0.56; P = .009), and at 24 weeks, including Part B score (Cohen d, 0.25; 95% CI, 0.01-0.49; P = .04) but not Part A score (Cohen d, 0.12; 95% CI, -0.05 to 0.28; P = .18). Improvements were observed in an observer-rated measure of persecutory delusions (PSYRATS delusion) at 12 weeks (Cohen d, 0.47; 95% CI, 0.17-0.78; P = .002) and 24 weeks (Cohen d, 0.50; 95% CI, 0.20-0.80; P = .001) and belief flexibility at 12 weeks (Cohen d, 0.29; 95% CI, 0.09-0.49; P = .004) and 24 weeks (Cohen d, 0.28; 95% CI, 0.08-0.49; P = .005). There were no significant effects on jumping to conclusions. Improved belief flexibility and worry mediated paranoia change (range mediated, 36%-56%).
Conclusions and relevance: SlowMo did not demonstrate significant improvements in the primary measure of paranoia at 24 weeks; however, a beneficial effect of SlowMo on paranoia was indicated by the results on the primary measure at an earlier point and on observer-rated paranoia and self-reported persecution at 12 and 24 weeks. Further work to optimize SlowMo's effects is warranted.
Trial registration: isrctn.org Identifier: ISRCTN 32448671.
Conflict of interest statement
Figures
References
-
- Schizophrenia Commission . The Abandoned Illness: A Report From the Schizophrenia Commission. Rethink Mental Illness; November 2012.
-
- Turner DT, Burger S, Smit F, Valmaggia LR, van der Gaag M. What constitutes sufficient evidence for case formulation–driven CBT for psychosis? cumulative meta-analysis of the effect on hallucinations and delusions. Schizophr Bull. 2020;46(5):1072-1085. doi:10.1093/schbul/sbaa045 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
