

Efficacy and Safety of Topical Timolol for the Treatment of Infantile Hemangioma in the Early Proliferative Stage: A Randomized Clinical Trial
- PMID: 33825828
- PMCID: PMC8027942
- DOI: 10.1001/jamadermatol.2021.0596
Efficacy and Safety of Topical Timolol for the Treatment of Infantile Hemangioma in the Early Proliferative Stage: A Randomized Clinical Trial
Abstract
Importance: Treatment of infantile hemangioma (IH) with topical timolol in the first 2 months of life (early proliferative phase) may prevent further growth and the need for treatment with oral propranolol. To our knowledge, no studies have determined whether beginning early treatment with timolol for IH is better than in other proliferative stages.
Objective: To evaluate the efficacy and safety of timolol maleate solution, 0.5%, for the early treatment of IH in infants younger than 60 days.
Design, setting, and participants: This multicenter, randomized, double-blind, placebo-controlled, phase 2a pilot clinical trial included patients aged 10 to 60 days with focal or segmental hemangiomas (superficial, deep, mixed, or minimal/arrested growth). Patients were randomly assigned to treatment with topical timolol maleate solution, 0.5%, or placebo twice daily for 24 weeks. Changes in lesion size (volume, thickness) and color were evaluated from photographs taken at 2, 4, 8, 12, 24, and 36 weeks. Vital signs and adverse effects were recorded at each visit. The study was carried out from November 2015 to January 2017, and data analyses were completed in September 2019.
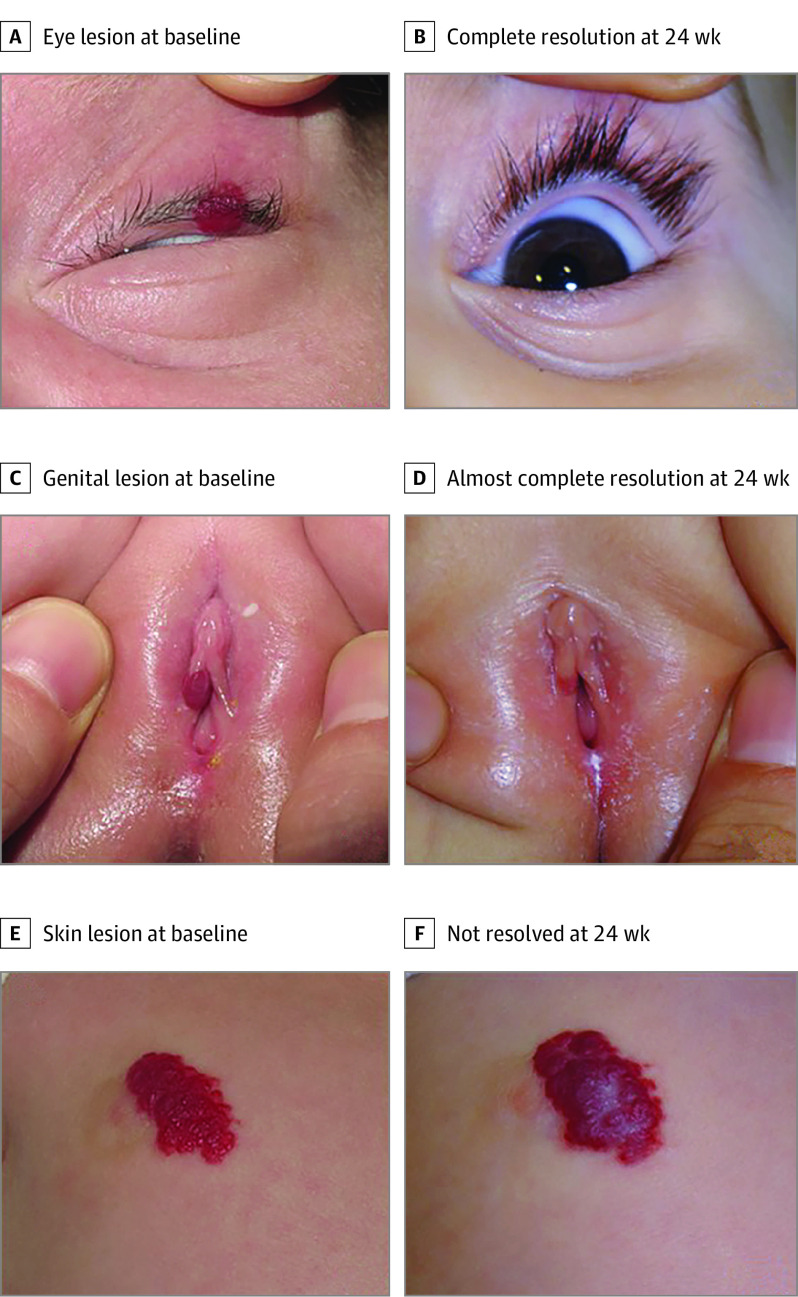
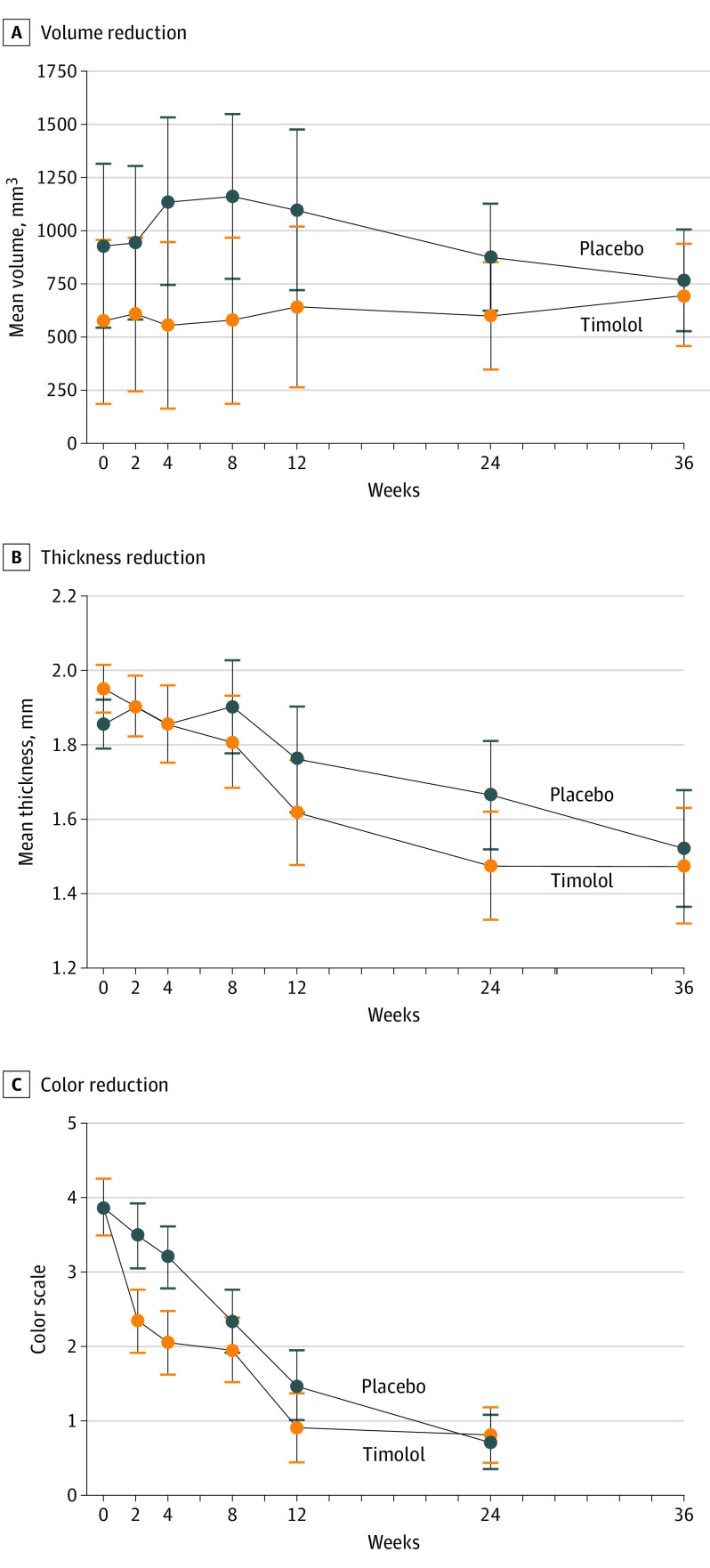
Main outcomes and measures: The primary outcome of complete or nearly complete IH resolution and the secondary outcomes of changes in lesion thickness, volume, and color were evaluated by a blinded investigator.
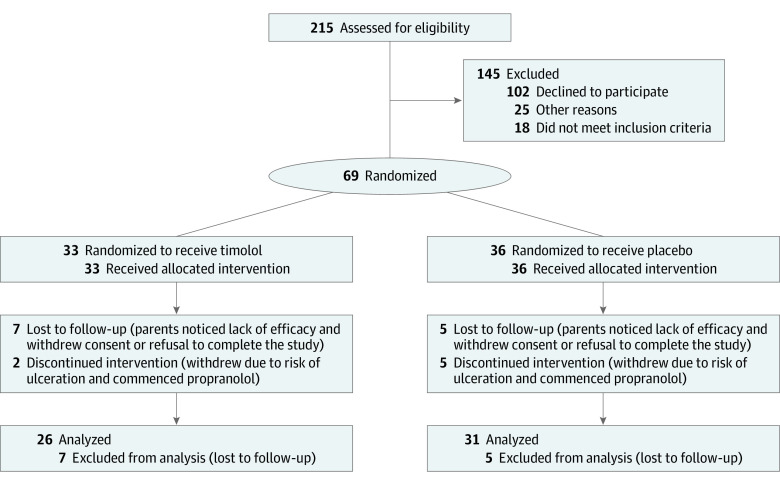
Results: Of the 69 patients recruited, the mean (SD) age was 48.4 (10.6) days; 55 (80%) were female; and 51 (74%), 11 (16%), 6 (9%), and 1 (1%) had superficial, mixed, abortive, or deep IHs, respectively. The IHs were localized, segmental, or indeterminate in 60 (87%), 7 (10%), and 2 (3%) patients, respectively. The IHs were located on the head and/or neck (n = 23 [33%]) or other body sites (n = 46 [67%]). The study was completed by 26 of 33 (79%) patients receiving timolol and 31 of 36 (86%) receiving placebo. There were no significant differences between timolol and placebo for complete or nearly complete IH resolution at 24 weeks (n = 11 [42%] vs n = 11 [36%]; P = .37). The odds ratio of complete or almost complete response vs no response at week 24 was 1.33 (95% CI, 0.45-3.89). There were no between-group differences in IH size (volume, thickness). An improvement in color was observed at week 4 in the timolol group, and timolol was well tolerated with no systemic adverse effects.
Conclusions and relevance: In this randomized clinical trial, results demonstrated that topical timolol is well tolerated for the treatment of early proliferative IH but provides limited benefit in lesion resolution when given during the early proliferative stage.
Trial registration: EudraCT Identifier: 2013-005199-17.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
