

Variation in Initial U.S. Hospital Responses to the Coronavirus Disease 2019 Pandemic
- PMID: 33826584
- PMCID: PMC8217146
- DOI: 10.1097/CCM.0000000000005013
Variation in Initial U.S. Hospital Responses to the Coronavirus Disease 2019 Pandemic
Abstract
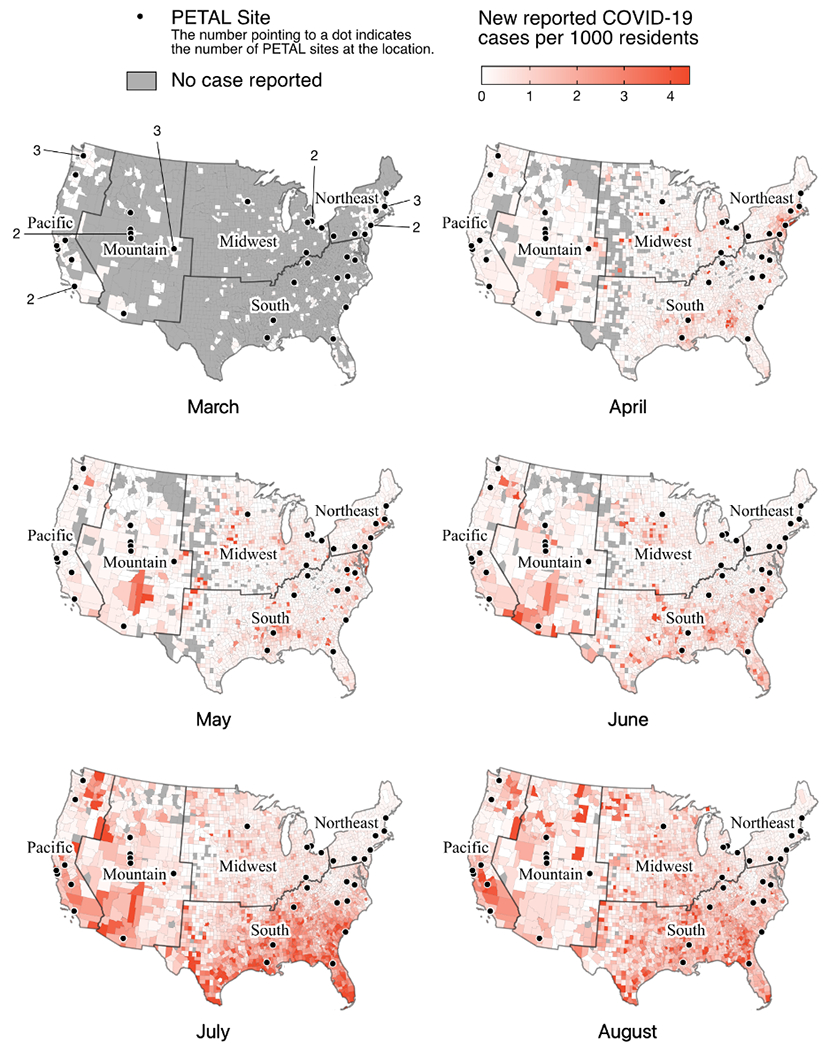
Objectives: The coronavirus disease 2019 pandemic has strained many healthcare systems. In response, U.S. hospitals altered their care delivery systems, but there are few data regarding specific structural changes. Understanding these changes is important to guide interpretation of outcomes and inform pandemic preparedness. We sought to characterize emergency responses across hospitals in the United States over time and in the context of local case rates early in the coronavirus disease 2019 pandemic.
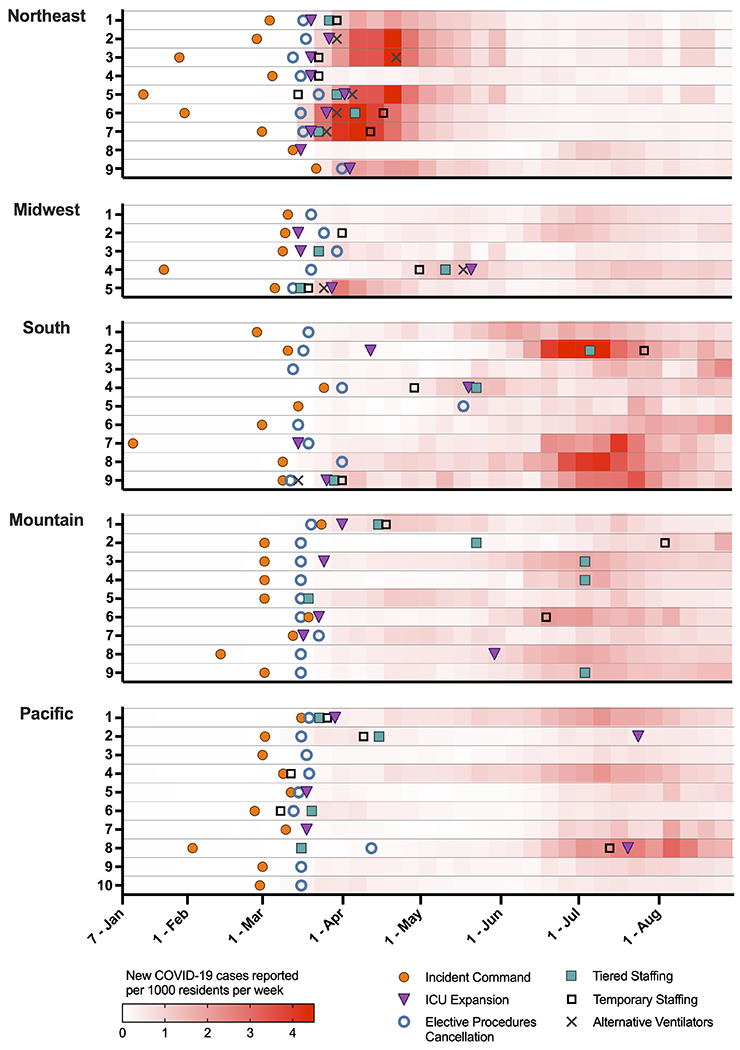
Design: We surveyed hospitals from a national acute care trials group regarding operational and structural changes made in response to the coronavirus disease 2019 pandemic from January to August 2020. We collected prepandemic characteristics and changes to hospital system, space, staffing, and equipment during the pandemic. We compared the timing of these changes with county-level coronavirus disease 2019 case rates.
Setting and participants: U.S. hospitals participating in the Prevention and Early Treatment of Acute Lung Injury Network Coronavirus Disease 2019 Observational study. Site investigators at each hospital collected local data.
Interventions: None.
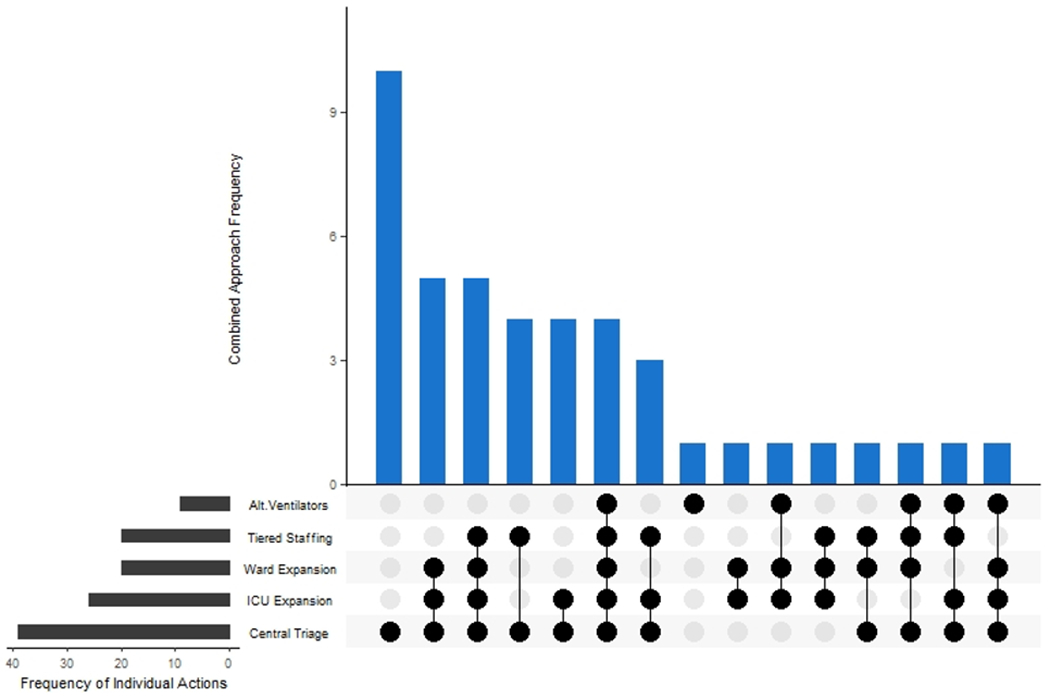
Measurements and main results: Forty-five sites participated (94% response rate). System-level changes (incident command activation and elective procedure cancellation) occurred at nearly all sites, preceding rises in local case rates. The peak inpatient census during the pandemic was greater than the prior hospital bed capacity in 57% of sites with notable regional variation. Nearly half (49%) expanded ward capacity, and 63% expanded ICU capacity, with nearly all bed expansion achieved through repurposing of clinical spaces. Two-thirds of sites adapted staffing to care for patients with coronavirus disease 2019, with 48% implementing tiered staffing models, 49% adding temporary physicians, nurses, or respiratory therapists, and 30% changing the ratios of physicians or nurses to patients.
Conclusions: The coronavirus disease 2019 pandemic prompted widespread system-level changes, but front-line clinical care varied widely according to specific hospital needs and infrastructure. Linking operational changes to care delivery processes is a necessary step to understand the impact of the coronavirus disease 2019 pandemic on patient outcomes.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Mathews reports grants from National Institutes of Health (NIH)/National Heart Lung and Blood Institute (NHBLI) (K23HL130648) and serves on a steering committee of A Multi-Center, Adaptive, Randomized, Double-blind, Placebo-controlled Study to Assess the Efficacy and Safety of Gimsilumab in Subjects With Lung Injury or Acute Respiratory Distress Syndrome Secondary to COVID-19 (BREATHE) trial, funded by Roivant/Kinevant Sciences, outside of the submitted work. Dr. Vranas reports support from the Veterans Affairs Portland Health Care System, outside the submitted work. Dr. Harhay reports editorial positions at the American Thoracic Society and receiving grants from the NIH, outside the submitted work. Dr. Chang reported receiving personal fees from PureTech and LaJolla Pharmaceuticals, outside the submitted work. Dr. Hough reports grants from the NIH during the conduct of the study. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Capacity Strain and Response During Coronavirus Disease 2019: One Size Does Not Fit All, and One Size Does Not Fit One.Crit Care Med. 2021 Jul 1;49(7):1189-1192. doi: 10.1097/CCM.0000000000005040. Crit Care Med. 2021. PMID: 33826585 No abstract available.
References
-
- Carenzo L, Costantini E, Greco M, et al.: Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy. Anaesthesia 2020; 75: 928–934. - PubMed
-
- U.S. Office of the Assistant Secretary of Preparedness and Response Hospital Preparedness Program. Healthcare Preparedness Capabilities: National Guidelines for Healthcare System Preparedness. Washington, D.C.: U.S. Department of Health and Human Services; 2012. Available from: https://www.phe.gov/preparedness/planning/hpp/reports/documents/capabili.... Accessed: 2020 Dec 17.
Publication types
MeSH terms
Grants and funding
- U01 HL123031/HL/NHLBI NIH HHS/United States
- U01 HL123020/HL/NHLBI NIH HHS/United States
- U01 HL123009/HL/NHLBI NIH HHS/United States
- K24 HL141526/HL/NHLBI NIH HHS/United States
- U01 HL123004/HL/NHLBI NIH HHS/United States
- K23 HL140165/HL/NHLBI NIH HHS/United States
- U01 HL123008/HL/NHLBI NIH HHS/United States
- U01 HL123022/HL/NHLBI NIH HHS/United States
- R01 HS028038/HS/AHRQ HHS/United States
- U01 HL123027/HL/NHLBI NIH HHS/United States
- U01 HL122998/HL/NHLBI NIH HHS/United States
- K23 HL130648/HL/NHLBI NIH HHS/United States
- U01 HL123018/HL/NHLBI NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- U01 HL122989/HL/NHLBI NIH HHS/United States
- R00 HL141678/HL/NHLBI NIH HHS/United States
- U01 HL123023/HL/NHLBI NIH HHS/United States
- IK2 HX003005/HX/HSRD VA/United States
- U01 HL123033/HL/NHLBI NIH HHS/United States
- U01 HL123010/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
