

Active surveillance of patients who have sentinel node positive melanoma: An international, multi-institution evaluation of adoption and early outcomes after the Multicenter Selective Lymphadenectomy Trial II (MSLT-2)
- PMID: 33826754
- PMCID: PMC8764513
- DOI: 10.1002/cncr.33483
Active surveillance of patients who have sentinel node positive melanoma: An international, multi-institution evaluation of adoption and early outcomes after the Multicenter Selective Lymphadenectomy Trial II (MSLT-2)
Abstract
Background: For patients with sentinel lymph node (SLN)-positive cutaneous melanoma, the Second Multicenter Selective Lymphadenectomy trial demonstrated equivalent disease-specific survival (DSS) with active surveillance using nodal ultrasound versus completion lymph node dissection (CLND). Adoption and outcomes of active surveillance in clinical practice and in adjuvant therapy recipients are unknown.
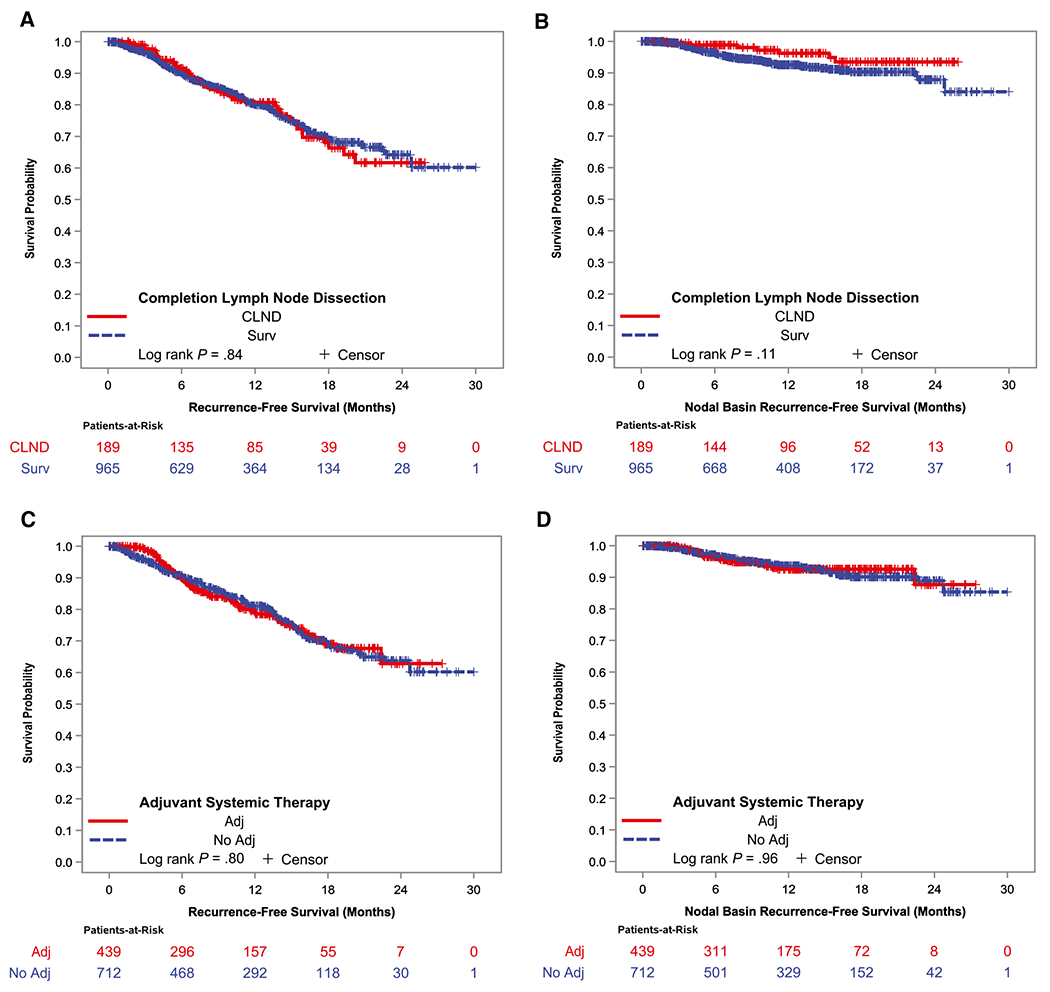
Methods: In a retrospective cohort of SLN-positive adults treated at 21 institutions in Australia, Europe, and the United States from June 2017 to November 2019, the authors evaluated the impact of active surveillance and adjuvant therapy on all-site recurrence-free survival (RFS), isolated nodal RFS, distant metastasis-free survival (DMFS), and DSS using Kaplan-Meier curves and Cox proportional hazard models.
Results: Among 6347 SLN biopsies, 1154 (18%) were positive and had initial negative distant staging. In total, 965 patients (84%) received active surveillance, 189 (16%) underwent CLND. Four hundred thirty-nine patients received adjuvant therapy (surveillance, 38%; CLND, 39%), with the majority (83%) receiving anti-PD-1 immunotherapy. After a median follow-up of 11 months, 220 patients developed recurrent disease (surveillance, 19%; CLND, 22%), and 24 died of melanoma (surveillance, 2%; CLND, 4%). Sixty-eight patients had an isolated nodal recurrence (surveillance, 6%; CLND, 4%). In patients who received adjuvant treatment without undergoing prior CLND, all isolated nodal recurrences were resectable. On risk-adjusted multivariable analyses, CLND was associated with improved isolated nodal RFS (hazard ratio [HR], 0.36; 95% CI, 0.15-0.88), but not all-site RFS (HR, 0.68; 95% CI, 0.45-1.02). Adjuvant therapy improved all-site RFS (HR, 0.52; 95% CI, 0.47-0.57). DSS and DMFS did not differ by nodal management or adjuvant treatment.
Conclusions: Active surveillance has been adopted for most SLN-positive patients. At initial assessment, real-world outcomes align with randomized trial findings, including in adjuvant therapy recipients.
Lay summary: For patients with melanoma of the skin and microscopic spread to lymph nodes, monitoring with ultrasound is an alternative to surgically removing the remaining lymph nodes. The authors studied adoption and real-world outcomes of ultrasound monitoring in over 1000 patients treated at 21 centers worldwide, finding that most patients now have ultrasounds instead of surgery. Although slightly more patients have cancer return in the lymph nodes with this strategy, typically, it can be removed with delayed surgery. Compared with up-front surgery, ultrasound monitoring results in the same overall risk of melanoma coming back at any location or of dying from melanoma.
Keywords: active surveillance; cohort studies; cutaneous malignant melanoma; follow-up studies; immunotherapy; lymph node excision; metastatic melanoma; sentinel lymph node.
© 2021 American Cancer Society.
Figures
Comment in
-
Active surveillance of patients who have melanoma with a positive sentinel node in an era of effective adjuvant therapy: Early lessons learned … and still learning.Cancer. 2021 Jul 1;127(13):2177-2180. doi: 10.1002/cncr.33484. Epub 2021 Apr 7. Cancer. 2021. PMID: 33826746 No abstract available.
References
-
- Wong SL, Morton DL, Thompson JF, et al. Melanoma patients with positive sentinel nodes who did not undergo completion lymphadenectomy: a multi-institutional study. Ann Surg Oncol. 2006;13:809–816. - PubMed
-
- Klemen ND, Han G, Leong SP, et al. Completion lymphadenectomy for a positive sentinel node biopsy in melanoma patients is not associated with a survival benefit. J Surg Oncol. 2019;119:1053–1059. - PubMed
-
- Leiter U, Buettner PG, Eigentler TK, Forschner A, Meier F, Garbe C. Is detection of melanoma metastasis during surveillance in an early phase of development associated with a survival benefit? Melanoma Res. 2010;20:240–246. - PubMed
-
- Leiter U, Stadler R, Mauch C, et al. Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): a multicentre, randomised, phase 3 trial. Lancet Oncol. 2016;17:757–767. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
