

Comparison of Patient Experience Between Primary Care Settings Tailored for Homeless Clientele and Mainstream Care Settings
- PMID: 33827104
- PMCID: PMC8567819
- DOI: 10.1097/MLR.0000000000001548
Comparison of Patient Experience Between Primary Care Settings Tailored for Homeless Clientele and Mainstream Care Settings
Abstract
Background: More than 1 million Americans receive primary care from federal homeless health care programs yearly. Vulnerabilities that can make care challenging include pain, addiction, psychological distress, and a lack of shelter. Research on the effectiveness of tailoring services for this population is limited.
Objective: The aim was to examine whether homeless-tailored primary care programs offer a superior patient experience compared with nontailored ("mainstream") programs overall, and for highly vulnerable patients.
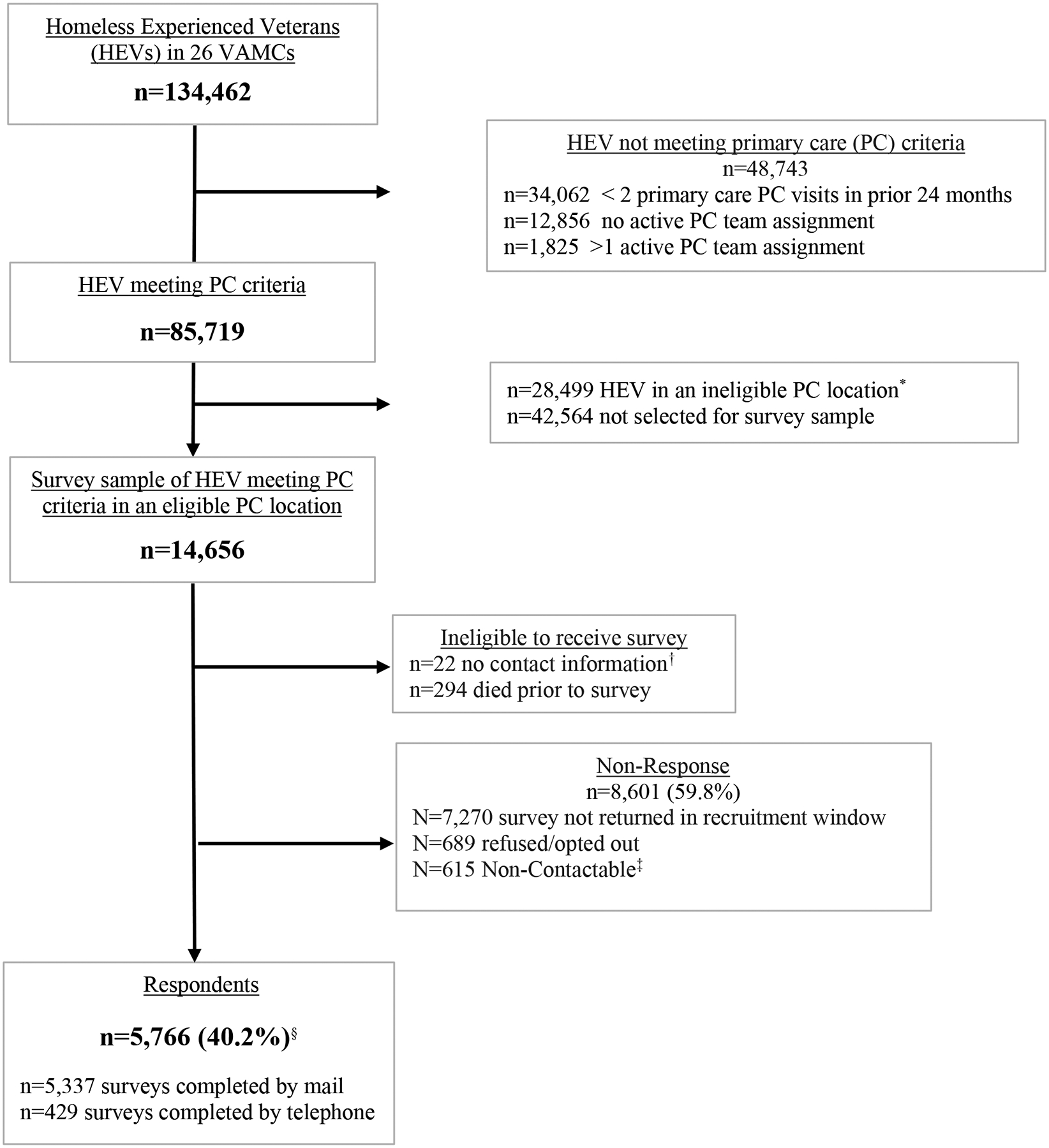
Research design: National patient survey comparing 26 US Department of Veterans Affairs (VA) Medical Centers' homeless-tailored primary care ("H-PACT"s) to mainstream primary care ("mainstream PACT"s) at the same locations.
Participants: A total of 5766 homeless-experienced veterans.
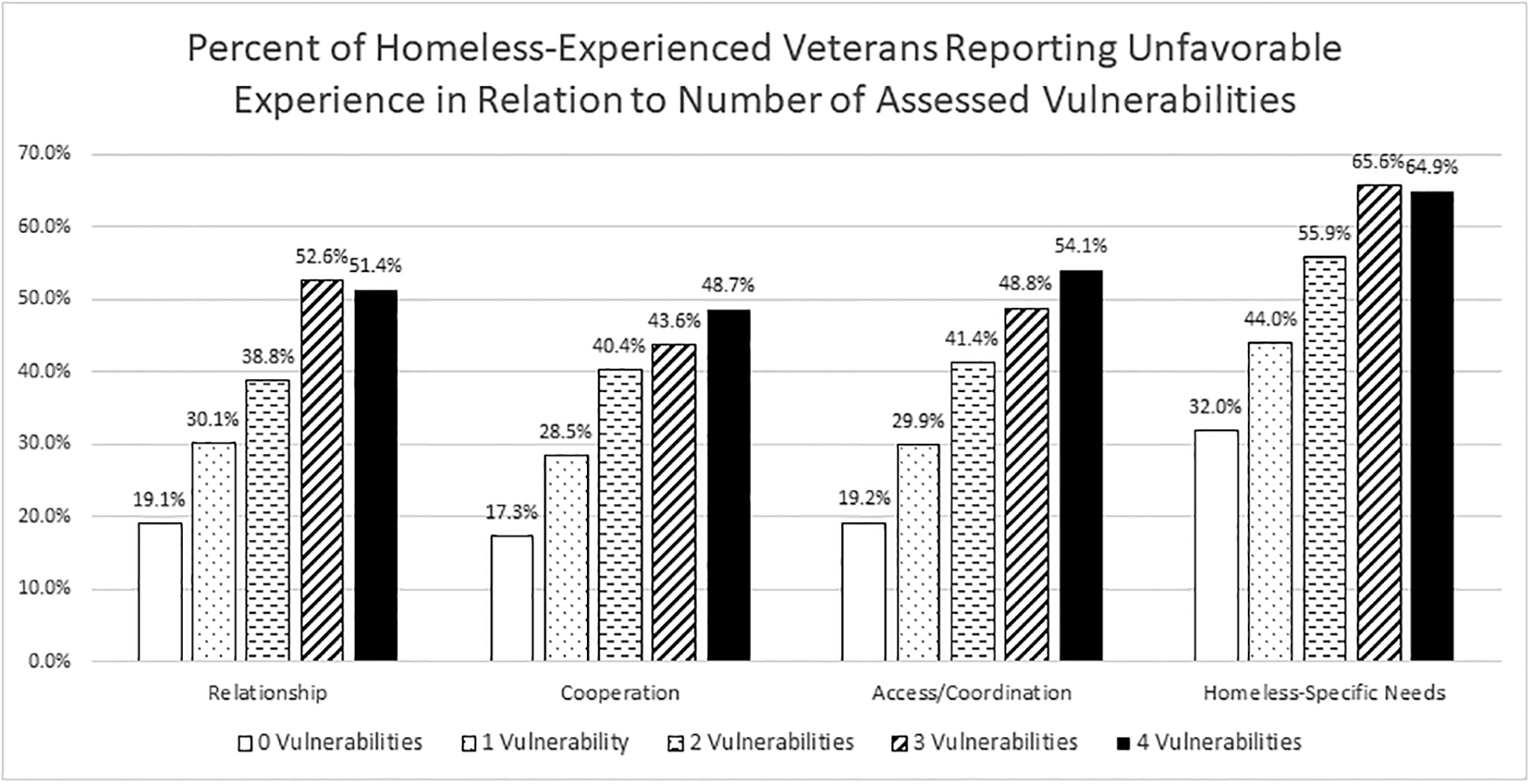
Measures: Primary care experience on 4 scales: Patient-Clinician Relationship, Cooperation, Accessibility/Coordination, and Homeless-Specific Needs. Mean scores (range: 1-4) were calculated and dichotomized as unfavorable versus not. We counted key vulnerabilities (chronic pain, unsheltered homelessness, severe psychological distress, and history of overdose, 0-4), and categorized homeless-experienced veterans as having fewer (≤1) and more (≥2) vulnerabilities.
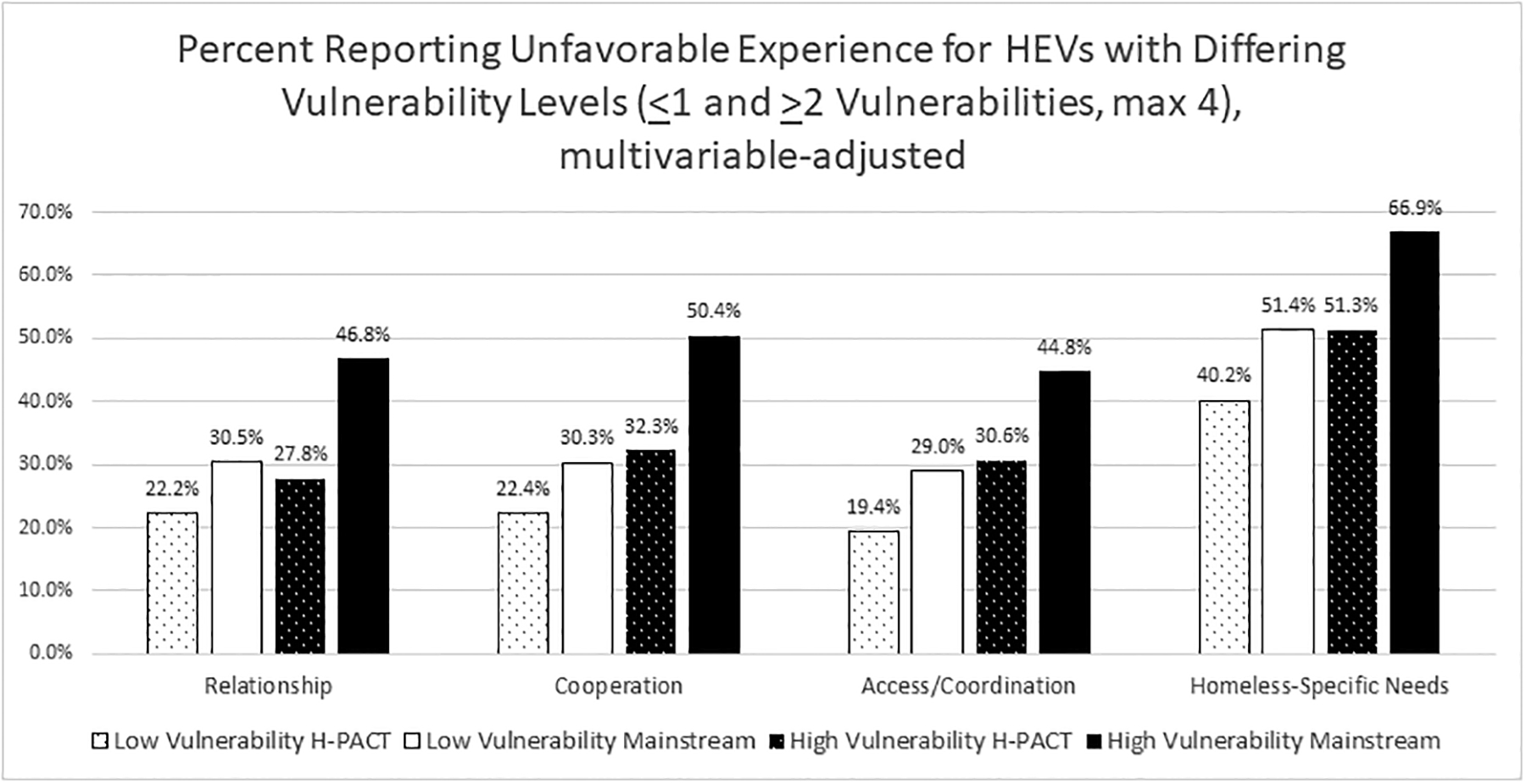
Results: H-PACTs outscored mainstream PACTs on all scales (all P<0.001). Unfavorable care experiences were more common in mainstream PACTs compared with H-PACTs, with adjusted risk differences of 11.9% (95% CI=6.3-17.4), 12.6% (6.2-19.1), 11.7% (6.0-17.3), and 12.6% (6.2-19.1) for Relationship, Cooperation, Access/Coordination, and Homeless-Specific Needs, respectively. For the Relationship and Cooperation scales, H-PACTs were associated with a greater reduction in unfavorable experience for patients with ≥2 vulnerabilities versus ≤1 (interaction P<0.0001).
Conclusions: Organizations that offer primary care for persons experiencing homelessness can improve the primary care experience by tailoring the design and delivery of services.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
All authors were financially affiliated with the United States Department of Veterans Affairs through employment or contract during the preparation of this manuscript. There are no other conflicts of interest relevant to the work under consideration. Outside of the submitted work, S.G.K. has financial relationships with UpToDate, Inc. and Thermo Fisher Scientific & Zimmer Biomet, and A.L.V. has a financial relationship Heart Rhythm Clinical and Research Solutions, as outlined in their Authorship Responsibility, Disclosure, and Copyright Transfer forms.
Figures
Similar articles
-
Comparing homeless persons' care experiences in tailored versus nontailored primary care programs.Am J Public Health. 2013 Dec;103 Suppl 2(Suppl 2):S331-9. doi: 10.2105/AJPH.2013.301481. Epub 2013 Oct 22. Am J Public Health. 2013. PMID: 24148052 Free PMC article.
-
Enhancing Primary Care Experiences for Homeless Patients with Serious Mental Illness: Results from a National Survey.J Prim Care Community Health. 2021 Jan-Dec;12:2150132721993654. doi: 10.1177/2150132721993654. J Prim Care Community Health. 2021. PMID: 33543675 Free PMC article.
-
Providing Positive Primary Care Experiences for Homeless Veterans Through Tailored Medical Homes: The Veterans Health Administration's Homeless Patient Aligned Care Teams.Med Care. 2019 Apr;57(4):270-278. doi: 10.1097/MLR.0000000000001070. Med Care. 2019. PMID: 30789541 Free PMC article.
-
Delivery of gender-sensitive comprehensive primary care to women veterans: implications for VA Patient Aligned Care Teams.J Gen Intern Med. 2014 Jul;29 Suppl 2(Suppl 2):S703-7. doi: 10.1007/s11606-013-2699-3. J Gen Intern Med. 2014. PMID: 24715395 Free PMC article. Review.
-
Review of Reported Adverse Events Occurring Among the Homeless Veteran Population in the Veterans Health Administration.J Patient Saf. 2021 Dec 1;17(8):e821-e828. doi: 10.1097/PTS.0000000000000884. J Patient Saf. 2021. PMID: 34406986 Review.
Cited by
-
A scoping review examining patient experience and what matters to people experiencing homelessness when seeking healthcare.BMC Health Serv Res. 2024 Apr 20;24(1):492. doi: 10.1186/s12913-024-10971-8. BMC Health Serv Res. 2024. PMID: 38643146 Free PMC article.
-
Staying safe, feeling welcome, being seen: How spatio-temporal configurations affect relations of care at an inclusive health and wellness centre.Health Expect. 2023 Dec;26(6):2620-2629. doi: 10.1111/hex.13858. Epub 2023 Sep 1. Health Expect. 2023. PMID: 37656503 Free PMC article.
-
Insights for Conducting Large-Scale Surveys with Veterans Who Have Experienced Homelessness.J Soc Distress Homeless. 2023;32(1):123-134. doi: 10.1080/10530789.2021.2013013. Epub 2021 Dec 28. J Soc Distress Homeless. 2023. PMID: 37234355 Free PMC article.
-
Material hardship, forced displacement, and negative health outcomes among unhoused people who use drugs in Los Angeles, California and Denver, Colorado: a latent class analysis.BMC Public Health. 2025 Feb 13;25(1):591. doi: 10.1186/s12889-025-21626-6. BMC Public Health. 2025. PMID: 39939965 Free PMC article.
-
What do Veterans with homeless experience want us to know that we are not asking? A qualitative content analysis of comments from a national survey of healthcare experience.Health Soc Care Community. 2022 Nov;30(6):e5027-e5037. doi: 10.1111/hsc.13918. Epub 2022 Jul 22. Health Soc Care Community. 2022. PMID: 35866310 Free PMC article.
References
-
- Office of Community Planning and Development. The 2018 Annual Homeless Assessment Report (AHAR) to Congress (Part 1). 2019; Available at: https://files.hudexchange.info/resources/documents/2018-AHAR-Part-1.pdf. Accessed May 15, 2020.
-
- Gelberg L, Linn LS. Psychological distress among homeless adults. J Nerv Ment Dis. 1989;177(5):291–295. - PubMed
-
- Midboe AM, Byrne T, Smelson D, Jasuja G, McInnes K, Troszak LK. The Opioid Epidemic In Veterans Who Were Homeless Or Unstably Housed. Health Aff (Millwood). 2019;38(8):1289–1297. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
