

Detection of parathyroid adenomas with multiphase 4DCT: towards a true four-dimensional technique
- PMID: 33827463
- PMCID: PMC8028189
- DOI: 10.1186/s12880-021-00597-1
Detection of parathyroid adenomas with multiphase 4DCT: towards a true four-dimensional technique
Abstract
Background: Four-dimensional computed tomography (4DCT) is a commonly performed examination in the management of primary hyperparathyroidism, combining three-dimensional imaging with enhancement over time as the fourth dimension. We propose a novel technique consisting of 16 different contrast phases instead of three or four different phases. The main aim of this study was to ascertain whether this protocol allows the detection of parathyroid adenomas within dose limits. Our secondary aim was to examine the enhancement of parathyroid lesions over time.
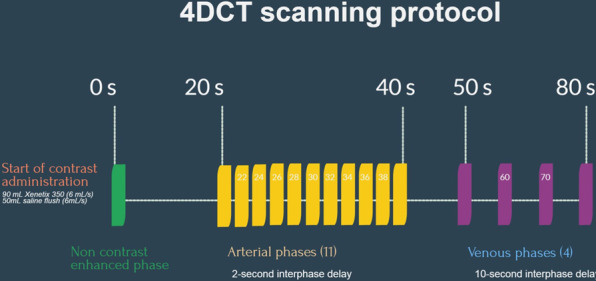
Methods: For this prospective study, we included 15 patients with primary hyperparathyroidism and a positive ultrasound prior to surgery. We performed 4DCT with 16 different phases: an unenhanced phase followed by 11 consecutive arterial phases and 4 venous phases. Continuous axial scanning centered on the thyroid was performed over a fixed 8 cm or 16 cm coverage volume after the start of contrast administration.
Results: In all patients, an enlarged parathyroid lesion was demonstrated, and the mean lesion size was 13.6 mm. The mean peak arterial enhancement for parathyroid lesions was 384 Hounsfield units (HU) compared to 333 HU for the normal thyroid. No significant difference could be found. The time to peak (TTP) was significantly earlier for parathyroid adenomas than for normal thyroid tissue: 30.8 s versus 32.3 s (p value 0.008). The mean slope of increase (MSI) of the enhancement curve was significantly steeper than that of normal thyroid tissue: 29.8% versus 22.2% (p value 0.012). The mean dose length product was 890.7 mGy cm with a calculated effective dose of 6.7 mSv.
Conclusion: Our 4DCT protocol may allow better visualization of the pattern of enhancement of parathyroid lesions, as enhancement over time curves can be drawn. In this way, wash-in and wash-out of contrast in suspected lesions can be readily demonstrated. Motion artifacts are less problematic as multiple phases are available. Exposure to our proposed 4DCT technique is comparable to that for classic helical 4DCT. Careful selection of parameters (lowering kV and SNR) can help to further reduce the dose.
Keywords: 4DCT; CT dose reduction; Endocrine disorders; Hyperparathyroidism; Parathyroid.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Bilezikian JP, Brandi ML, Eastell R, Silverberg SJ, Udelsman R, Marcocci C, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. J Clin Endocrinol Metab. 2014;99(10):3561–3569. doi: 10.1210/jc.2014-1413. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
