

Image-guided microwave ablation of hepatocellular carcinoma (≤5.0 cm): is MR guidance more effective than CT guidance?
- PMID: 33827464
- PMCID: PMC8028080
- DOI: 10.1186/s12885-021-08099-7
Image-guided microwave ablation of hepatocellular carcinoma (≤5.0 cm): is MR guidance more effective than CT guidance?
Abstract
Background: Given their widespread availability and relatively low cost, percutaneous thermal ablation is commonly performed under the guidance of computed tomography (CT) or ultrasound (US). However, such imaging modalities may be restricted due to insufficient image contrast and limited tumor visibility, which results in imperfect intraoperative treatment or an increased risk of damage to critical anatomical structures. Currently, magnetic resonance (MR) guidance has been proven to be a possible solution to overcome the above shortcomings, as it provides more reliable visualization of the target tumor and allows for multiplanar capabilities, making it the modality of choice. Unfortunately, MR-guided ablation is limited to specialized centers, and the cost is relatively high. Is ablation therapy under MR guidance better than that under CT guidance? This study retrospectively compared the efficacy of CT-guided and MR-guided microwave ablation (MWA) for the treatment of hepatocellular carcinoma (HCC ≤ 5.0 cm).
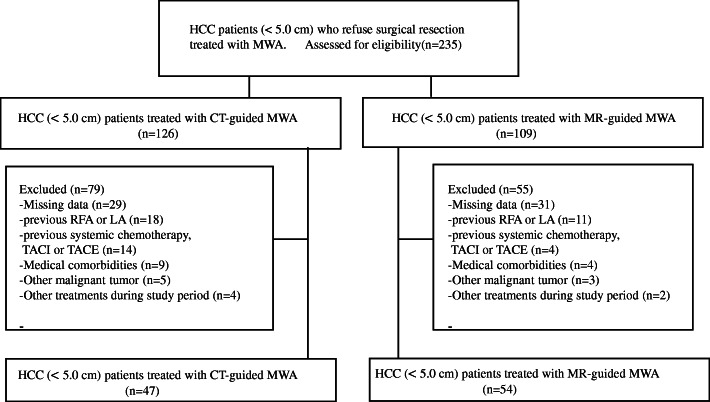
Methods: In this retrospective study, 47 patients and 54 patients received MWA under the guidance of CT and MR, respectively. The inclusion criteria were a single HCC ≤ 5.0 cm or a maximum of three. The local tumor progression (LTP), overall survival (OS), prognostic factors for local progression, and safety of this technique were assessed.
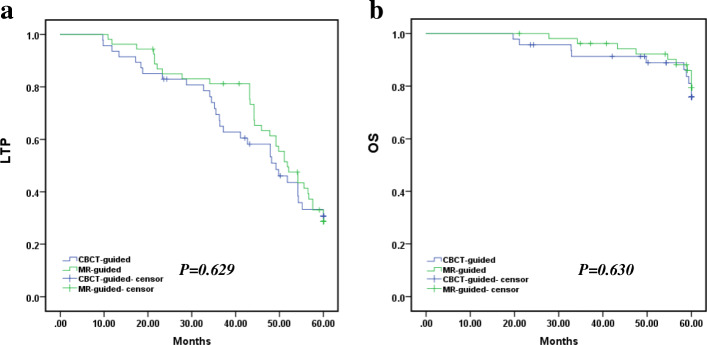
Results: All procedures were technically successful. The complication rates of the two groups were remarkably different with respect to incidences of liver abscess and pleural effusion (P < 0.05). The mean LTP was 44.264 months in the CT-guided group versus 47.745 months in the MR-guided group of HCC (P = 0.629, log-rank test). The mean OS was 56.772 months in the patients who underwent the CT-guided procedure versus 58.123 months in those who underwent the MR-guided procedure (P = 0.630, log-rank test). Multivariate Cox regression analysis further illustrated that tumor diameter (< 3 cm) and the number of lesions (single) were important factors affecting LTP and OS.
Conclusions: Both CT-guided and MR-guided MWA are comparable therapies for the treatment of HCC (< 5 cm), and there was no difference in survival between the two groups. However, MR-guided MWA could reduce the incidence of complications.
Keywords: Hepatocellular carcinoma; Interventional radiology; Magnetic resonance imaging; Microwave ablation.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
MR-guided microwave ablation of hepatocellular carcinoma (HCC): is general anesthesia more effective than local anesthesia?BMC Cancer. 2021 May 17;21(1):562. doi: 10.1186/s12885-021-08298-2. BMC Cancer. 2021. PMID: 34001036 Free PMC article.
-
Comparison of Microwave and Radiofrequency Ablation for the Treatment of Small- and Medium-Sized Hepatocellular Carcinomas in a Prospective Randomized Trial.Rofo. 2024 May;196(5):482-490. doi: 10.1055/a-2203-2733. Epub 2023 Dec 8. Rofo. 2024. PMID: 38065541 Clinical Trial. English.
-
Comparative Study of Application of Computed Tomography/Ultrasound and Computed Tomography Imaging Guidance Methods in the Microwave Ablation of Liver Cancer.J Comput Assist Tomogr. 2023 Jan-Feb 01;47(1):24-30. doi: 10.1097/RCT.0000000000001375. Epub 2022 Sep 1. J Comput Assist Tomogr. 2023. PMID: 36055224 Free PMC article.
-
Comparison of microwave ablation and radiofrequency ablation for hepatocellular carcinoma: a systematic review and meta-analysis.Int J Hyperthermia. 2019;36(1):264-272. doi: 10.1080/02656736.2018.1562571. Epub 2019 Jan 24. Int J Hyperthermia. 2019. PMID: 30676100
-
Ultrasound fusion imaging technologies for guidance in ablation therapy for liver cancer.J Med Ultrason (2001). 2020 Apr;47(2):257-263. doi: 10.1007/s10396-020-01006-w. Epub 2020 Feb 8. J Med Ultrason (2001). 2020. PMID: 32125577 Review.
Cited by
-
Interventional Magnetic Resonance Imaging Suite (IMRIS): How to build and how to use.Radiol Med. 2022 Oct;127(10):1063-1067. doi: 10.1007/s11547-022-01537-x. Epub 2022 Aug 26. Radiol Med. 2022. PMID: 36018489
-
Surgery or Percutaneous Ablation for Liver Tumors? The Key Points Are: When, Where, and How Large.Cancers (Basel). 2025 Apr 16;17(8):1344. doi: 10.3390/cancers17081344. Cancers (Basel). 2025. PMID: 40282520 Free PMC article.
-
Interventional oncology of liver tumors: how it all started and where are we now.Br J Radiol. 2022 Sep 1;95(1138):20220434. doi: 10.1259/bjr.20220434. Epub 2022 Jul 12. Br J Radiol. 2022. PMID: 35776630 Free PMC article. Review.
-
Recent Advances in Ablative Therapies for HCC.J Clin Exp Hepatol. 2025 Sep-Oct;15(5):102592. doi: 10.1016/j.jceh.2025.102592. Epub 2025 May 17. J Clin Exp Hepatol. 2025. PMID: 40535845 Review.
-
Efficacy and safety of computed tomography-guided microwave ablation with fine needle-assisted puncture positioning technique for hepatocellular carcinoma.World J Gastrointest Oncol. 2022 Sep 15;14(9):1727-1738. doi: 10.4251/wjgo.v14.i9.1727. World J Gastrointest Oncol. 2022. PMID: 36187402 Free PMC article.
References
-
- Mazzaferro V, Llovet JM, Miceli R, Bhoori S, Schiavo M, Mariani L, Camerini T, Roayaie S, Schwartz ME, Grazi GL, Adam R, Neuhaus P, Salizzoni M, Bruix J, Forner A, de Carlis L, Cillo U, Burroughs AK, Troisi R, Rossi M, Gerunda GE, Lerut J, Belghiti J, Boin I, Gugenheim J, Rochling F, van Hoek B, Majno P, Metroticket Investigator Study Group Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10(1):35–43. doi: 10.1016/S1470-2045(08)70284-5. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
