

Long-term oncologic result of laparoscopic versus open gastrectomy for gastric cancer: a propensity score matching analysis
- PMID: 33827601
- PMCID: PMC8028734
- DOI: 10.1186/s12957-021-02217-2
Long-term oncologic result of laparoscopic versus open gastrectomy for gastric cancer: a propensity score matching analysis
Abstract
Background: Laparoscopic gastrectomy is an acceptable procedure for early-stage gastric cancer; however, most patients are diagnosed at an advanced stage and older age in Taiwan. The feasibility and safety of applying laparoscopic gastrectomy in daily practice remain unclear. This study aimed to examine the short- and long-term outcomes of laparoscopic gastrectomy versus open procedures.
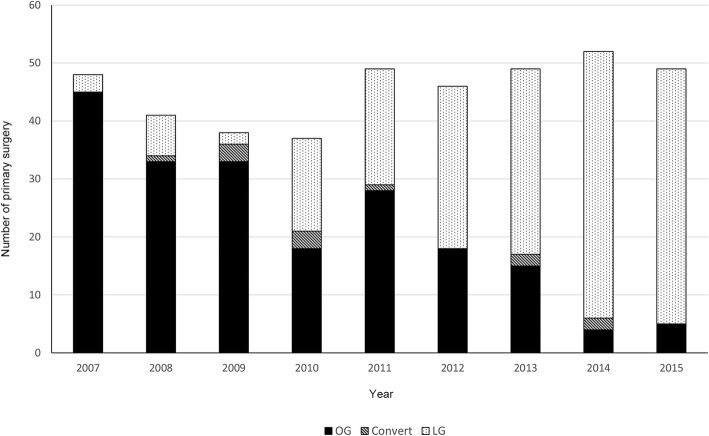
Methods: From 2007 to 2015, 192 patients who underwent open gastrectomy and 189 patients who underwent laparoscopic gastrectomy for gastric cancer at a single center were included. Propensity score matching analysis was used to adjust selection biases associated with age, preoperative hemoglobin, the extent of resection, tumor size, and stage of the disease. The demographics, perioperative parameters, short-term postoperative results, and 5-year survival data were analyzed.
Results: Open gastrectomy was more frequently performed in the elderly, larger tumor size, advanced stage of the disease, and disease requiring total gastrectomy or combined organ resection. After propensity score matching, 108 patients with laparoscopic gastrectomy were compared to 108 patients with open gastrectomy. The morbidity rates were not different in both groups (25.9%), while hospital stay was shorter in the laparoscopic group (16.0 vs. 18.8 days, p = 0.04). The 5-year overall survival and disease-free survival were superior in the laparoscopic group (p = 0.03 and p = 0.01, respectively); however, the survival differences were not significant in the subgroup analysis by stage. Laparoscopic gastrectomy had fewer recurrences than open gastrectomy. The pattern of recurrence was not different between the groups.
Conclusions: Laparoscopic gastrectomy can be safely applied in both early and locally advanced gastric cancer without compromising oncologic outcomes.
Trial registration: Retrospective registration.
Keywords: Gastric cancer; Laparoscopic surgery; Postoperative complications; Recurrence; Survival.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Kooby DA. Laparoscopic surgery for cancer: historical, theoretical, and technical considerations. Oncology (Williston Park) 2006;20:917–927. - PubMed
-
- Huscher CG, Mingoli A, Sgarzini G, Sansonetti A, Di Paola M, Recher A, Ponzano C. Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: five-year results of a randomized prospective trial. Ann Surg. 2005;241(2):232–237. doi: 10.1097/01.sla.0000151892.35922.f2. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
