

Is Fluoxetine Good for Subacute Stroke? A Meta-Analysis Evidenced From Randomized Controlled Trials
- PMID: 33828519
- PMCID: PMC8019826
- DOI: 10.3389/fneur.2021.633781
Is Fluoxetine Good for Subacute Stroke? A Meta-Analysis Evidenced From Randomized Controlled Trials
Abstract
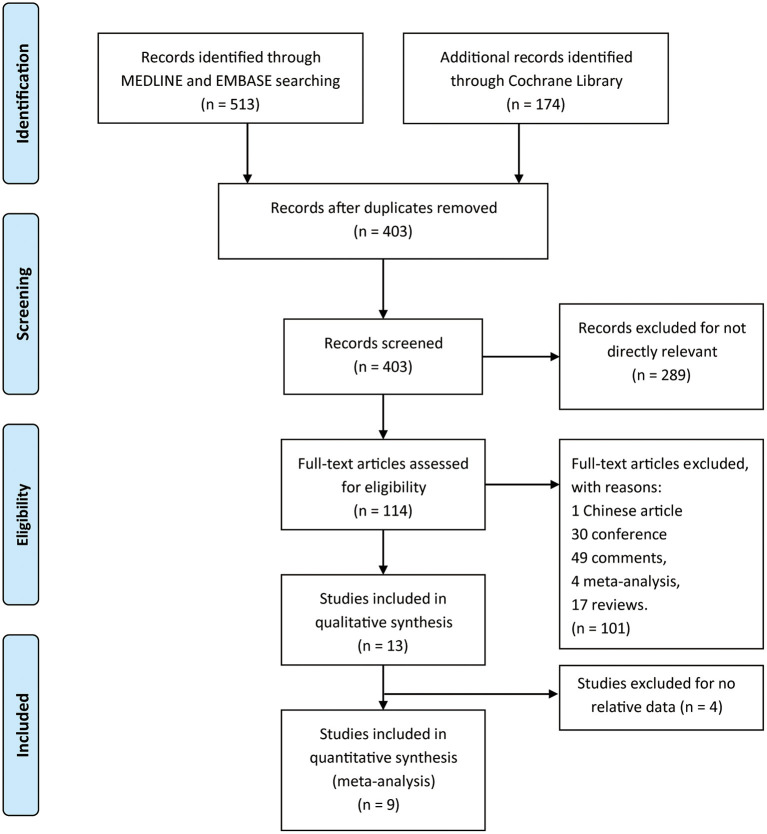
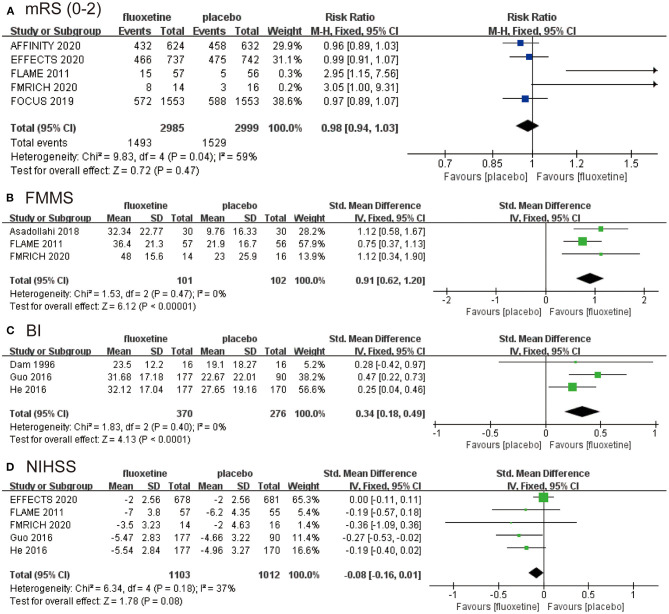
Background and Purpose: Fluoxetine is a drug commonly used to treat mental disorders, such as depression and obsessive-compulsive disorder, and some studies have shown that fluoxetine can improve motor and function recovery after stroke. Therefore, we performed a meta-analysis to investigate the efficacy and safety of fluoxetine in the treatment of post-stroke neurological recovery. Methods: PubMed, Embase, and Cochrane Library were searched for randomized controlled trials (RCTs) that were performed to assess the efficacy and safety of fluoxetine for functional and motor recovery in subacute stroke patients up to October 2020. Review Manager 5.3 software was used to assess the data. The risk ratio (RR) and standardized mean difference (SMD) were analyzed and calculated with a fixed effects model. Results: We pooled 6,788 patients from nine RCTs. The primary endpoint was modified Rankin Scale (mRS). Fluoxetine did not change the proportion of mRS ≤ 2 (P = 0.47). The secondary endpoints were Fugl-Meyer Motor Scale (FMMS), Barthel Index (BI), and National Institutes of Health Stroke Scale (NIHSS). Fluoxetine improved the FMMS (P < 0.00001) and BI(P < 0.0001) and showed a tendency of improving NIHSS (P = 0.08). In addition, we found that fluoxetine reduced the rate of new-onset depression (P < 0.0001) and new antidepressants (P < 0.0001). Conclusion: In post-stroke treatment, fluoxetine did not improve participants' mRS and NIHSS but improved FMMS and BI. This difference could result from heterogeneities between the trials: different treatment duration, clinical scales sensitivity, patient age, delay of inclusion, and severity of the deficit.
Keywords: MRS; fluoxetine; meta-analysis; recovery; rehabilitation; stroke.
Copyright © 2021 Liu, Yang, Xue, Chen, Wu, Yan, Wang, Wu, Chen and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The efficacy and safety of fluoxetine versus placebo for stroke recovery: a meta-analysis of randomized controlled trials.Int J Clin Pharm. 2023 Aug;45(4):839-846. doi: 10.1007/s11096-023-01573-1. Epub 2023 Apr 20. Int J Clin Pharm. 2023. PMID: 37081168 Review.
-
Recovery in Stroke Patients Treated With Fluoxetine Versus Placebo: A Pooled Analysis of 7,165 Patients.Neurologist. 2023 Mar 1;28(2):104-116. doi: 10.1097/NRL.0000000000000451. Neurologist. 2023. PMID: 35777860
-
Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trial.Lancet Neurol. 2011 Feb;10(2):123-30. doi: 10.1016/S1474-4422(10)70314-8. Epub 2011 Jan 7. Lancet Neurol. 2011. PMID: 21216670 Clinical Trial.
-
Safety and Efficacy of Stem Cell Therapy in Ischemic Stroke: A Comprehensive Systematic Review and Meta-Analysis.J Clin Med. 2025 Mar 20;14(6):2118. doi: 10.3390/jcm14062118. J Clin Med. 2025. PMID: 40142929 Free PMC article. Review.
-
Individual patient data meta-analysis of the effects of fluoxetine on functional outcomes after acute stroke.Int J Stroke. 2024 Aug;19(7):798-808. doi: 10.1177/17474930241242628. Epub 2024 Apr 8. Int J Stroke. 2024. PMID: 38497332 Free PMC article.
Cited by
-
State of the Art and Future of Stem Cell Therapy in Ischemic Stroke: Why Don't We Focus on Their Administration?Bioengineering (Basel). 2023 Jan 14;10(1):118. doi: 10.3390/bioengineering10010118. Bioengineering (Basel). 2023. PMID: 36671691 Free PMC article. Review.
-
Association between gut microbiota and post-stroke depression in Chinese population: A meta-analysis.Heliyon. 2022 Dec 22;8(12):e12605. doi: 10.1016/j.heliyon.2022.e12605. eCollection 2022 Dec. Heliyon. 2022. PMID: 36619429 Free PMC article.
-
The efficacy and safety of fluoxetine versus placebo for stroke recovery: a meta-analysis of randomized controlled trials.Int J Clin Pharm. 2023 Aug;45(4):839-846. doi: 10.1007/s11096-023-01573-1. Epub 2023 Apr 20. Int J Clin Pharm. 2023. PMID: 37081168 Review.
-
Evaluating the Effectiveness of Neuroprotective Strategies in Enhancing Post-stroke Recovery: A Systematic Review of Meta-Analyses and Clinical Trials.Cureus. 2024 Oct 12;16(10):e71343. doi: 10.7759/cureus.71343. eCollection 2024 Oct. Cureus. 2024. PMID: 39534815 Free PMC article. Review.
References
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. . Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2018) 49:e46–e110. 10.1016/j.jvs.2018.04.007 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources