

Subtrochanteric femur fractures: current review of management
- PMID: 33828858
- PMCID: PMC8022017
- DOI: 10.1302/2058-5241.6.200048
Subtrochanteric femur fractures: current review of management
Abstract
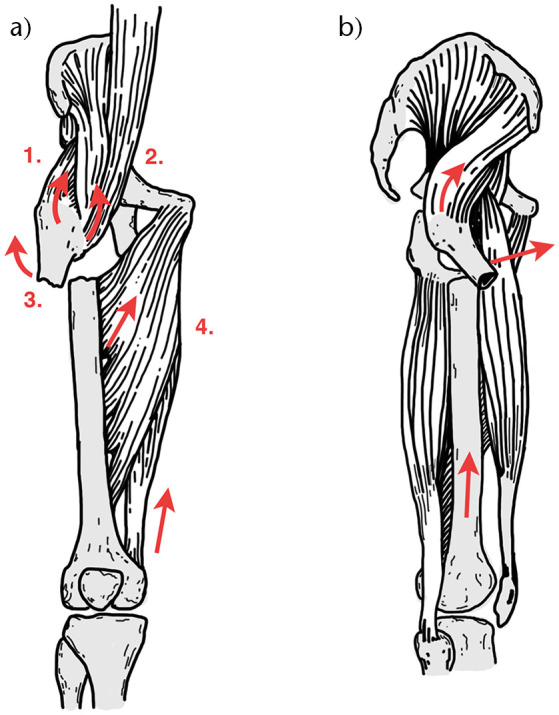
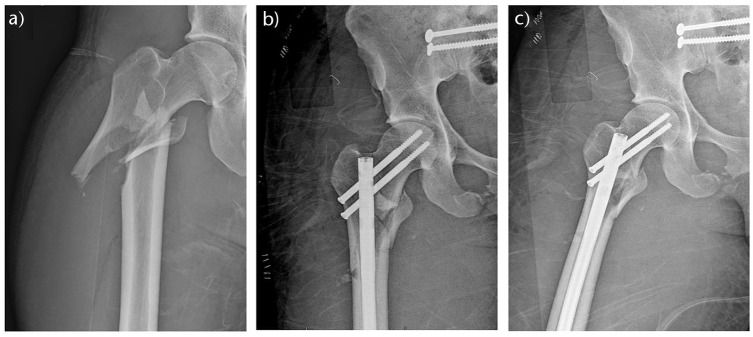
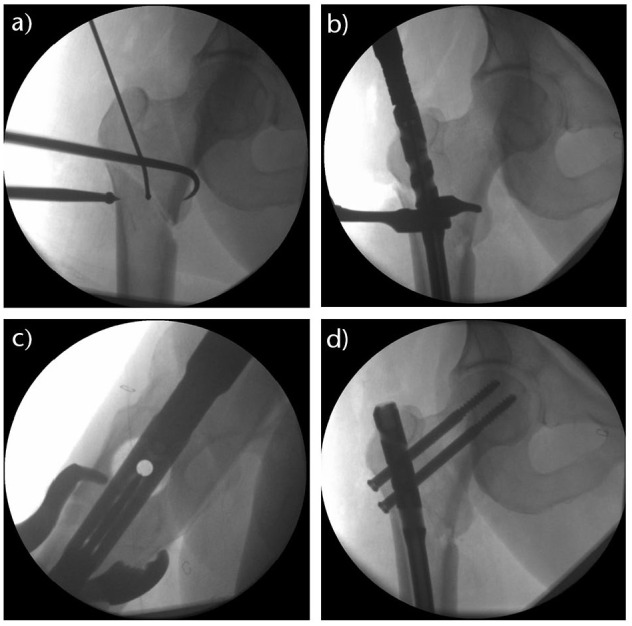
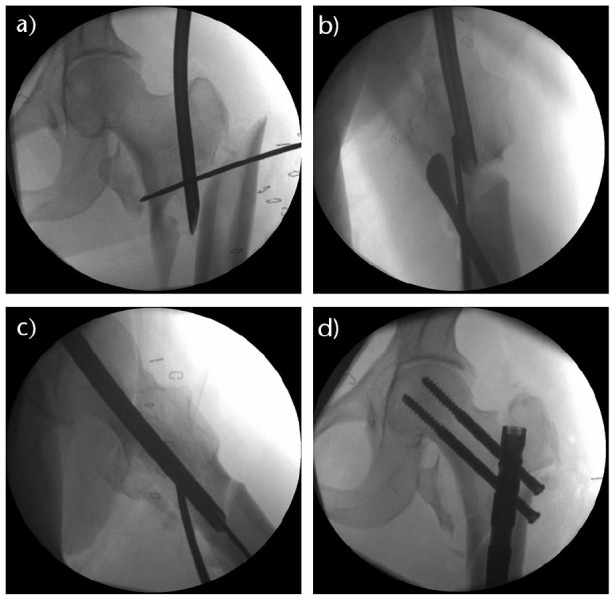
Subtrochanteric (ST) femur fractures are proximal femur fractures, which are often difficult to manage effectively because of their deforming anatomical forces.Operative management of ST fractures is the mainstay of treatment, with the two primary surgical implant options being intramedullary (IM) nails and extramedullary plates.Of these, IM nails have a biologic and biomechanical superiority, and have become the gold standard for ST femur fractures.The orthopaedic surgeon should become familiar and facile with several reduction techniques to create anatomical alignment in all unique ST fracture patterns.This article presents a comprehensive and current review of the epidemiology, anatomy, biomechanics, clinical presentation, diagnosis, and management of subtrochanteric femur fractures. Cite this article: EFORT Open Rev 2021;6:145-151. DOI: 10.1302/2058-5241.6.200048.
Keywords: femur; intramedullary nail; reduction techniques; subtrochanteric fracture.
© 2021 The author(s).
Conflict of interest statement
ICMJE Conflict of interest statement: The other authors declare no conflict of interest relevant to this work.
Figures
References
-
- Joglekar SB, Lindvall EM, Martirosian A. Contemporary management of subtrochanteric fractures. Orthop Clin North Am 2015;46:21–35. - PubMed
-
- Dell RM, Adams AL, Greene DF, et al. . Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res 2012;27:2544–2550. - PubMed
-
- Koch JC. The laws of bone architecture. Am J Anat 1917;21:177–211.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
