

P14/ARF-Positive Malignant Pleural Mesothelioma: A Phenotype With Distinct Immune Microenvironment
- PMID: 33828993
- PMCID: PMC8019896
- DOI: 10.3389/fonc.2021.653497
P14/ARF-Positive Malignant Pleural Mesothelioma: A Phenotype With Distinct Immune Microenvironment
Abstract
Introduction: The CDKN2A gene plays a central role in the pathogenesis of malignant pleural mesothelioma (MPM). The gene encodes for two tumor suppressor proteins, p16/INK4A and p14/ARF, frequently lost in MPM tumors. The exact role of p14/ARF in MPM and overall its correlation with the immune microenvironment is unknown. We aimed to determine whether there is a relationship between p14/ARF expression, tumor morphological features, and the inflammatory tumor microenvironment.
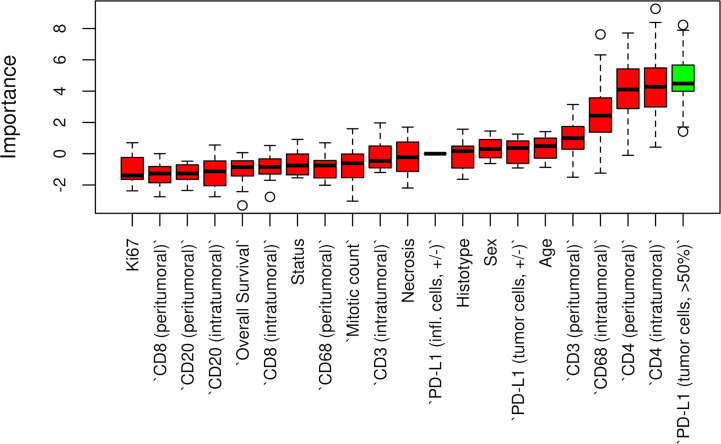
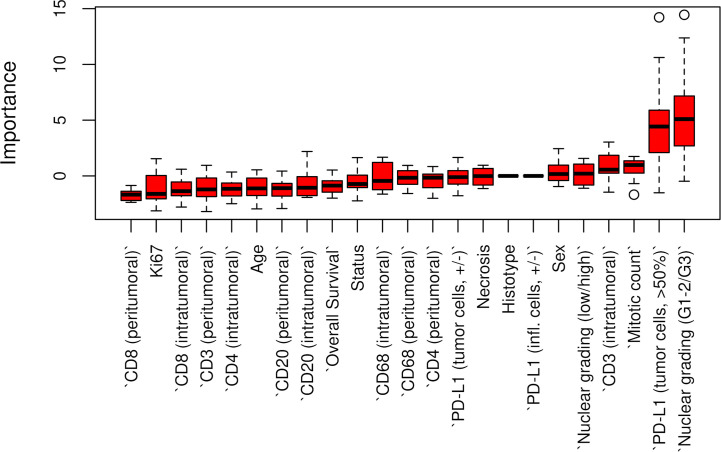
Methods: Diagnostic biopsies from 76 chemo-naive MPMs were evaluated. Pathological assessments of histotype, necrosis, inflammation, grading, and mitosis were performed. We evaluated p14/ARF, PD-L1 (tumor proportion score, TPS), and Ki-67 (percentage) by immunohistochemistry. Inflammatory cell components (CD3+, CD4+, CD8+ T lymphocytes; CD20+ B-lymphocytes; CD68+ and CD163+ macrophages) were quantified as percentages of positive cells, distinguishing between intratumoral and peritumoral areas. The expression of p14/ARF was associated with several clinical and pathological characteristics. A random forest-based machine-learning algorithm (Boruta) was implemented to identify which variables were associated with p14/ARF expression.
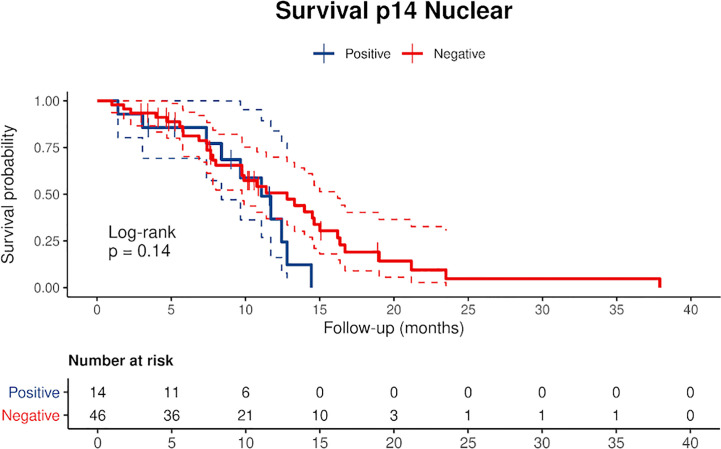
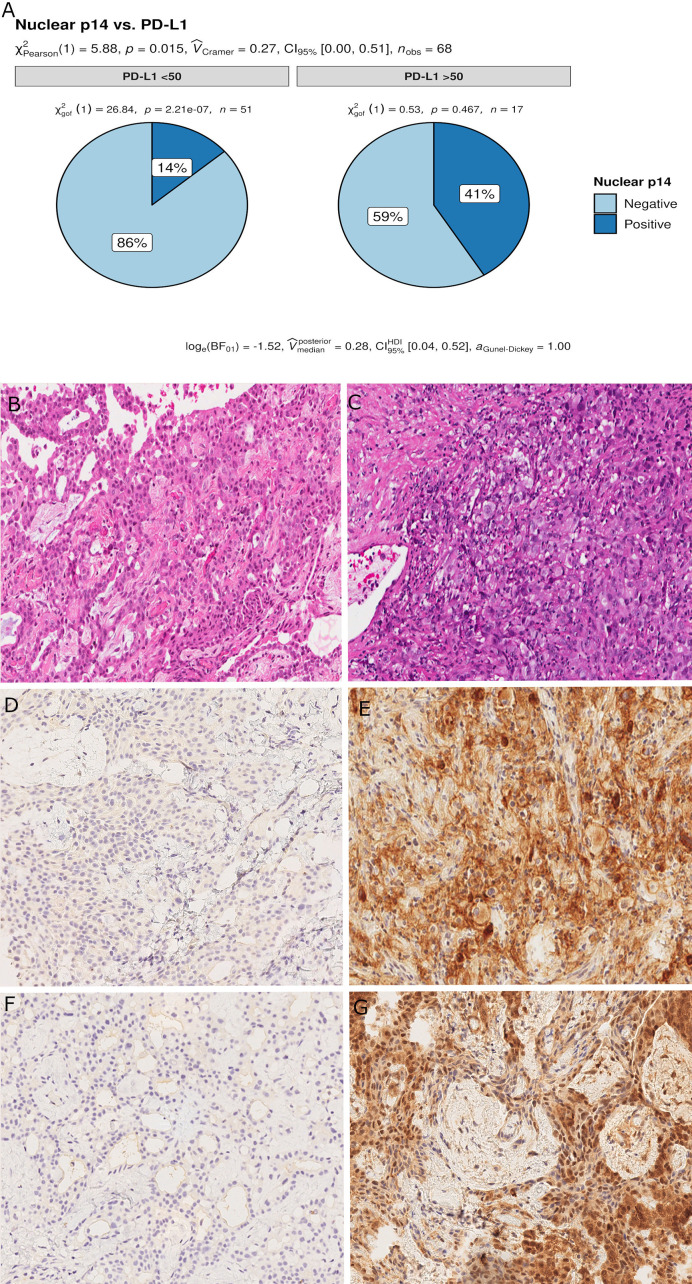
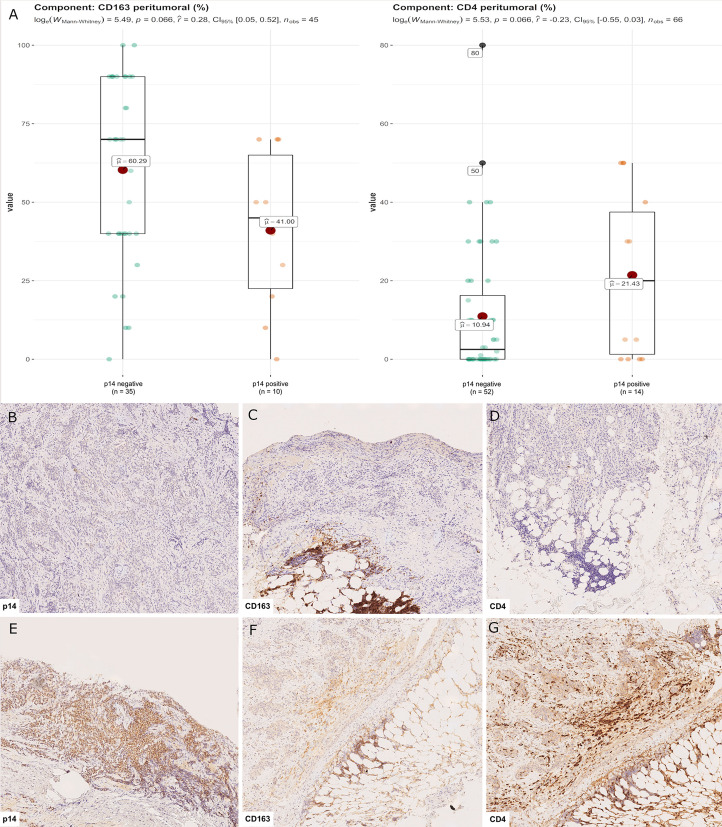
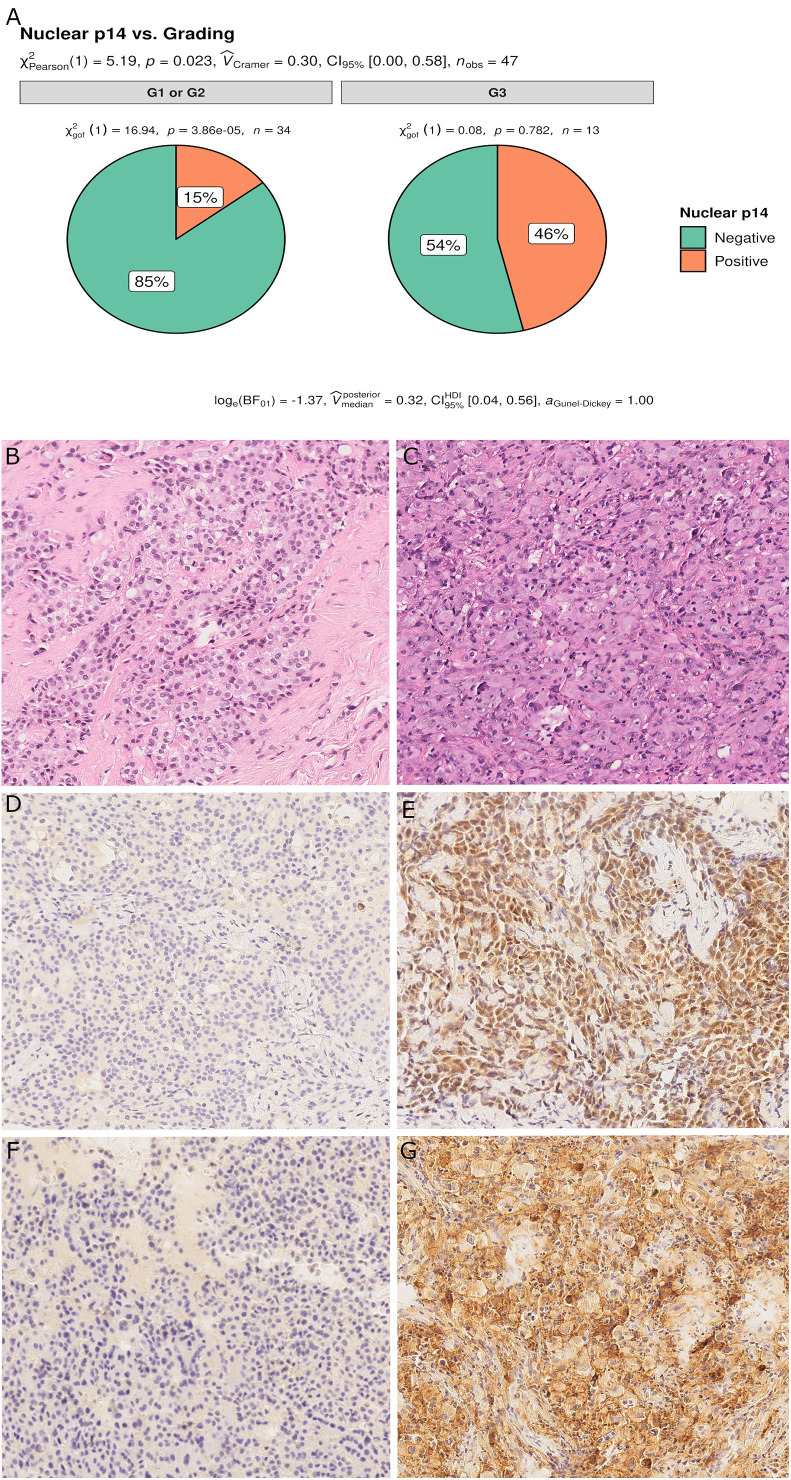
Results: p14/ARF was evaluated in 68 patients who had a sufficient number of tumor cells. Strong positivity was detected in 14 patients (21%) (11 epithelioid and 3 biphasic MPMs). At univariate analysis, p14/ARF-positive epithelioid mesotheliomas showed higher nuclear grade (G3) (p = 0.023) and higher PD-L1 expression (≥50%) (p = 0.042). The percentages of CD4 and CD163 in peritumoral areas were respectively higher and lower in p14/ARF positive tumors but did not reach statistical significance with our sample size (both p = 0.066). The Boruta algorithm confirmed the predictive value of PD-L1 percentage for p14/ARF expression in all histotypes.
Conclusions: p14/ARF-positive epithelioid mesotheliomas may mark a more aggressive pathological phenotype (higher nuclear grade and PD-L1 expression). Considering the results regarding the tumor immune microenvironment, p14/ARF-negative tumors seem to have an immune microenvironment less sensitive to immune checkpoint inhibitors, being associated with low PD-L1 and CD4 expression, and high CD163 percentage. The association between p14/ARF-positive MPMs and PD-L1 expression suggests a possible interaction of the two pathways. Confirmation of our preliminary results could be important for patient selection and recruitment in future clinical trials with anticancer immunotherapy.
Keywords: MPM; immune microenvironment; malignant pleural mesothelioma; p14/ARF; tumor microenvironment.
Copyright © 2021 Pezzuto, Lunardi, Vedovelli, Fortarezza, Urso, Grosso, Ceresoli, Kern, Vlacic, Faccioli, Schiavon, Gregori, Rea, Pasello and Calabrese.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous