

Can a Higher Protein/Low Glycemic Index vs. a Conventional Diet Attenuate Changes in Appetite and Gut Hormones Following Weight Loss? A 3-Year PREVIEW Sub-study
- PMID: 33829034
- PMCID: PMC8019730
- DOI: 10.3389/fnut.2021.640538
Can a Higher Protein/Low Glycemic Index vs. a Conventional Diet Attenuate Changes in Appetite and Gut Hormones Following Weight Loss? A 3-Year PREVIEW Sub-study
Abstract
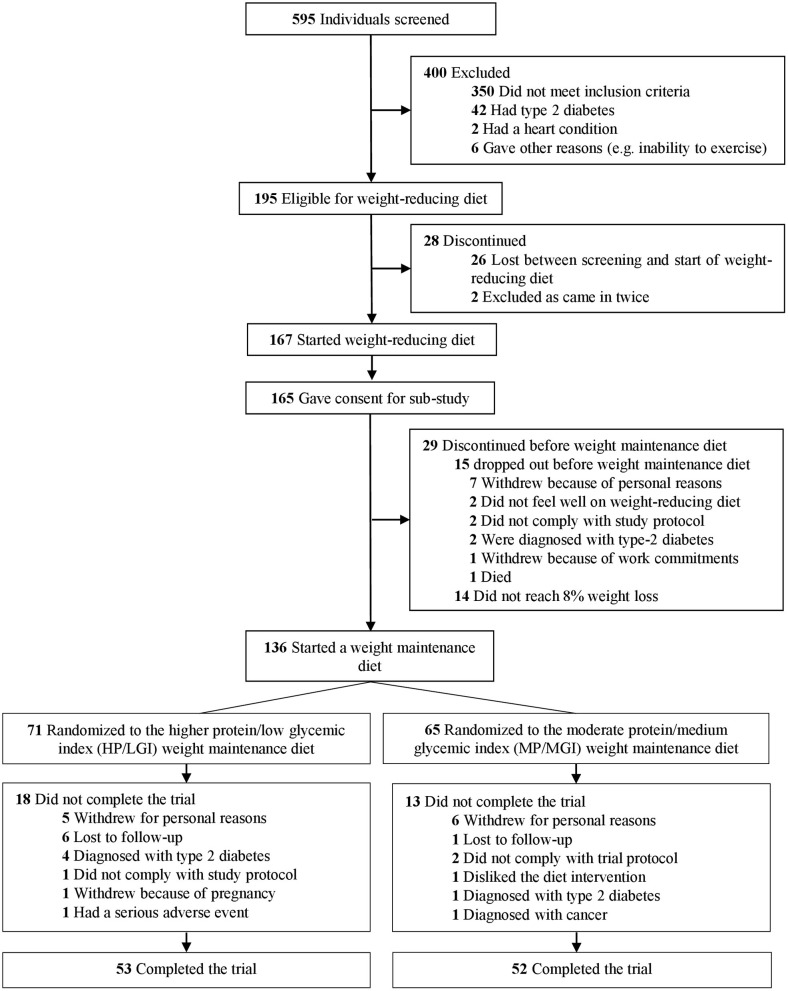
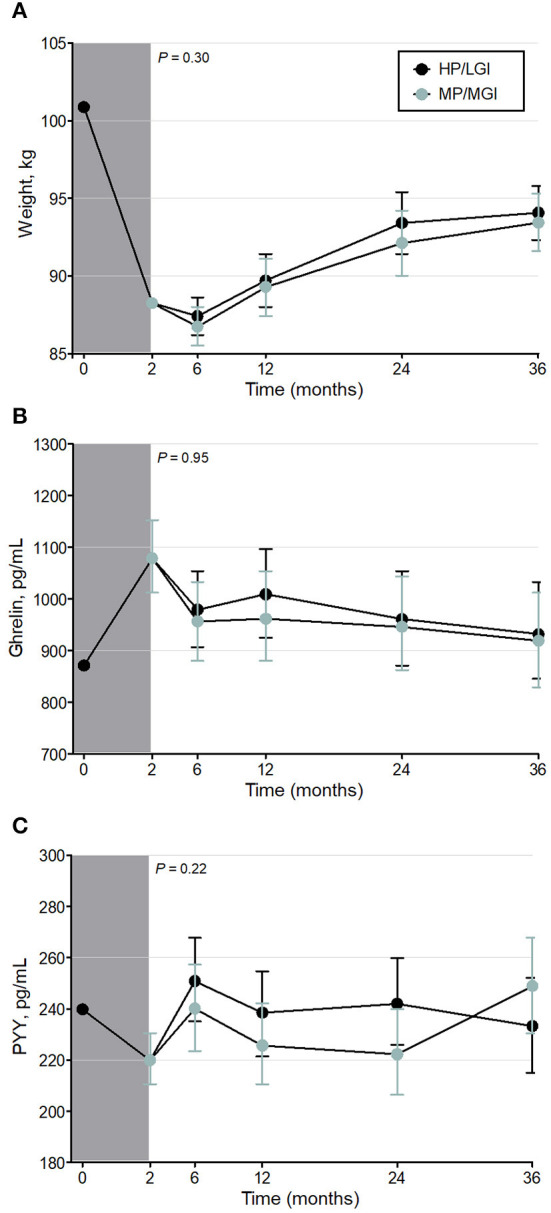
Background: Previous research showed that weight-reducing diets increase appetite sensations and/or circulating ghrelin concentrations for up to 36 months, with transient or enduring perturbations in circulating concentrations of the satiety hormone peptide YY. Objective: This study assessed whether a diet that is higher in protein and low in glycemic index (GI) may attenuate these changes. Methods: 136 adults with pre-diabetes and a body mass index of ≥25 kg/m2 underwent a 2-month weight-reducing total meal replacement diet. Participants who lost ≥8% body weight were randomized to one of two 34-month weight-maintenance diets: a higher-protein and moderate-carbohydrate (CHO) diet with low GI, or a moderate-protein and higher-CHO diet with moderate GI. Both arms involved recommendations to increase physical activity. Fasting plasma concentrations of total ghrelin and total peptide YY, and appetite sensations, were measured at 0 months (pre-weight loss), at 2 months (immediately post-weight loss), and at 6, 12, 24, and 36 months. Results: There was a decrease in plasma peptide YY concentrations and an increase in ghrelin after the 2-month weight-reducing diet, and these values approached pre-weight-loss values by 6 and 24 months, respectively (P = 0.32 and P = 0.08, respectively, vs. 0 months). However, there were no differences between the two weight-maintenance diets. Subjective appetite sensations were not affected by the weight-reducing diet nor the weight-maintenance diets. While participants regained an average of ~50% of the weight they had lost by 36 months, the changes in ghrelin and peptide YY during the weight-reducing phase did not correlate with weight regain. Conclusion: A higher-protein, low-GI diet for weight maintenance does not attenuate changes in ghrelin or peptide YY compared with a moderate-protein, moderate-GI diet. Clinical Trial Registry: ClinicalTrials.gov registry ID NCT01777893 (PREVIEW) and ID NCT02030249 (Sub-study).
Keywords: appetite; ghrelin; gut hormones; peptide YY; weight maintenance.
Copyright © 2021 Buso, Seimon, McClintock, Muirhead, Atkinson, Brodie, Dodds, Zibellini, Das, Wild-Taylor, Burk, Fogelholm, Raben, Brand-Miller and Sainsbury.
Conflict of interest statement
RS serves on the Nestlé Health Science Optifast® VLCDTM™ Advisory Board. JB-M is the President of the Glycemic Index Foundation (a non-profit food endorsement program), oversees a glycemic index testing service at the University of Sydney and is the author of books about the glycemic index, food and healthy eating. AS owns 50% of the shares in Zuman International, a company which receives royalties for books she has written about weight management and payments for presentations at industry conferences. She has also received presentation fees and travel reimbursements from Eli Lilly and Co, the Pharmacy Guild of Australia, Novo Nordisk, the Dietitians Association of Australia, Shoalhaven Family Medical Centres, the Pharmaceutical Society of Australia, and Metagenics, and served on the Nestlé Health Science Optifast VLCD advisory board from 2016 to 2018. FA is a director of the Glycemic Index Foundation (a non-profit food endorsement program), manages a glycemic index testing service at the University of Sydney, and is a co-author of books about the glycemic index. Finally, Cambridge Weight Plan©, Ltd, UK provided all meal replacement products used at all sites of the PREVIEW Study. The commercial and funding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, nor in the decision to publish the results. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A High-Protein, Low Glycemic Index Diet Suppresses Hunger but Not Weight Regain After Weight Loss: Results From a Large, 3-Years Randomized Trial (PREVIEW).Front Nutr. 2021 Jun 1;8:685648. doi: 10.3389/fnut.2021.685648. eCollection 2021. Front Nutr. 2021. PMID: 34141717 Free PMC article.
-
Associations of quantity and quality of carbohydrate sources with subjective appetite sensations during 3-year weight-loss maintenance: Results from the PREVIEW intervention study.Clin Nutr. 2022 Jan;41(1):219-230. doi: 10.1016/j.clnu.2021.11.038. Epub 2021 Dec 3. Clin Nutr. 2022. PMID: 34915273 Clinical Trial.
-
Post-weight loss changes in fasting appetite- and energy balance-related hormone concentrations and the effect of the macronutrient content of a weight maintenance diet: a randomised controlled trial.Eur J Nutr. 2021 Aug;60(5):2603-2616. doi: 10.1007/s00394-020-02438-3. Epub 2020 Dec 2. Eur J Nutr. 2021. PMID: 33263788 Free PMC article. Clinical Trial.
-
Brain somatic cross-talk: ghrelin, leptin and ultimate challengers of obesity.Nutr Neurosci. 2005 Feb;8(1):1-5. doi: 10.1080/10284150400027107. Nutr Neurosci. 2005. PMID: 15909762 Review.
-
Is glycemic index of food a feasible predictor of appetite, hunger, and satiety?J Nutr Sci Vitaminol (Tokyo). 2009 Jun;55(3):201-7. doi: 10.3177/jnsv.55.201. J Nutr Sci Vitaminol (Tokyo). 2009. PMID: 19602827 Review.
Cited by
-
A High-Protein, Low Glycemic Index Diet Suppresses Hunger but Not Weight Regain After Weight Loss: Results From a Large, 3-Years Randomized Trial (PREVIEW).Front Nutr. 2021 Jun 1;8:685648. doi: 10.3389/fnut.2021.685648. eCollection 2021. Front Nutr. 2021. PMID: 34141717 Free PMC article.
-
Fasting appetite-related gut hormone responses after weight loss induced by calorie restriction, exercise, or both in people with overweight or obesity: a meta-analysis.Int J Obes (Lond). 2025 May;49(5):776-792. doi: 10.1038/s41366-025-01726-4. Epub 2025 Feb 10. Int J Obes (Lond). 2025. PMID: 39929932 Free PMC article.
-
Effect of Dietary Approaches on Glycemic Control in Patients with Type 2 Diabetes: A Systematic Review with Network Meta-Analysis of Randomized Trials.Nutrients. 2023 Jul 15;15(14):3156. doi: 10.3390/nu15143156. Nutrients. 2023. PMID: 37513574 Free PMC article.
-
Obesity-induced and weight-loss-induced physiological factors affecting weight regain.Nat Rev Endocrinol. 2023 Nov;19(11):655-670. doi: 10.1038/s41574-023-00887-4. Epub 2023 Sep 11. Nat Rev Endocrinol. 2023. PMID: 37696920 Review.
-
Body weight regulation models in humans: insights for testing their validity.Nat Rev Endocrinol. 2025 Jul 24. doi: 10.1038/s41574-025-01149-1. Online ahead of print. Nat Rev Endocrinol. 2025. PMID: 40707700 Review.
References
-
- Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. . Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. The Lancet. (2017) 390:2627–42. 10.1016/S0140-6736(17)32129-3 - DOI - PMC - PubMed
-
- Klein S, Sheard NF, Pi-Sunyer X, Daly A, Wylie-Rosett J, Kulkarni K, et al. . Weight management through lifestyle modification for the prevention and management of type 2 diabetes: rationale and strategies: a statement of the American Diabetes Association, the North American Association for the Study of Obesity, and the American Society for Clinical Nutrition. Diabetes Care. (2004) 27:2067–73. 10.2337/diacare.27.8.2067 - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical