

Epidemiology of Marginal Zone Lymphoma
- PMID: 33829216
- PMCID: PMC8020862
- DOI: 10.21037/aol-20-28
Epidemiology of Marginal Zone Lymphoma
Abstract
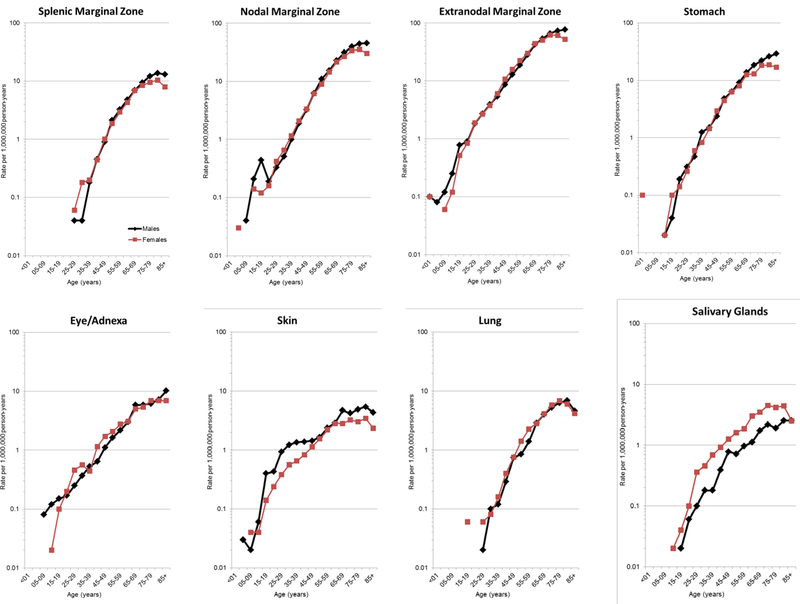
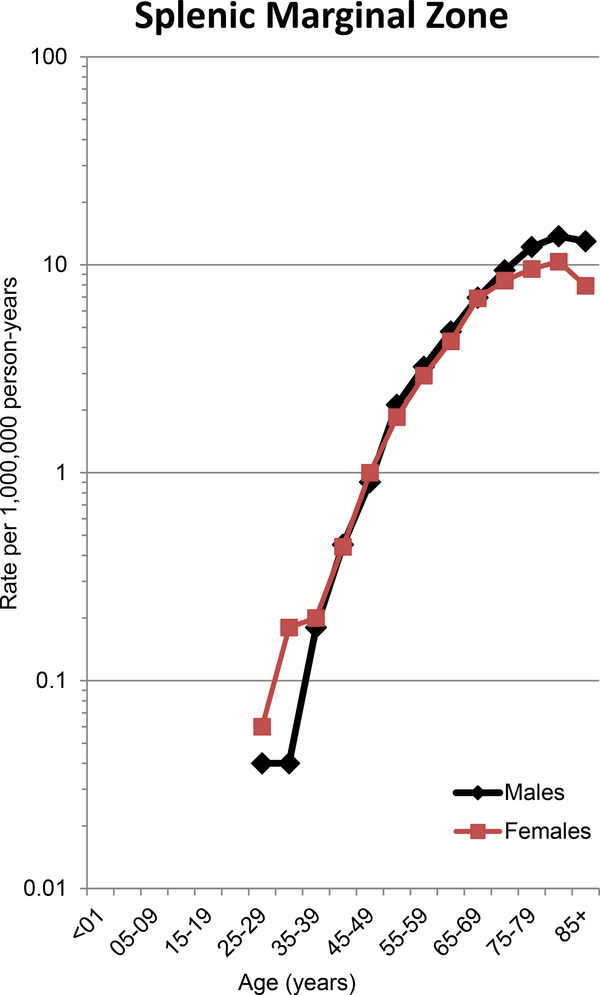
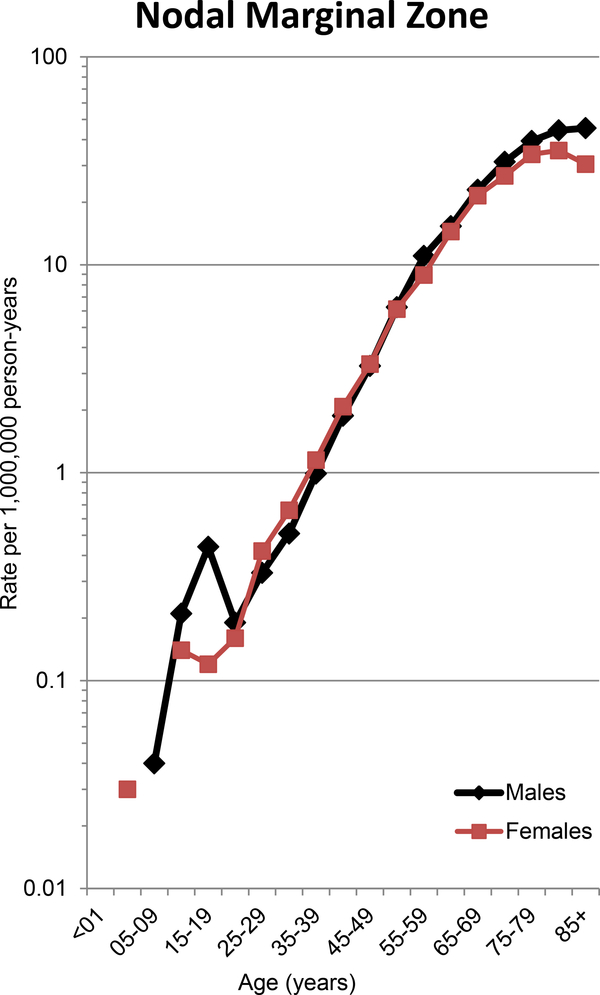
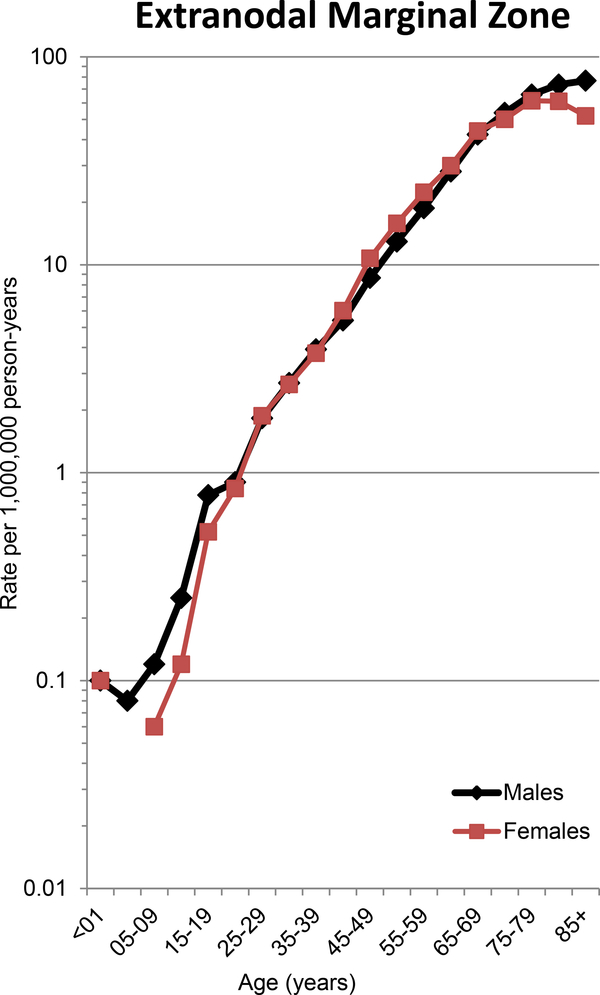
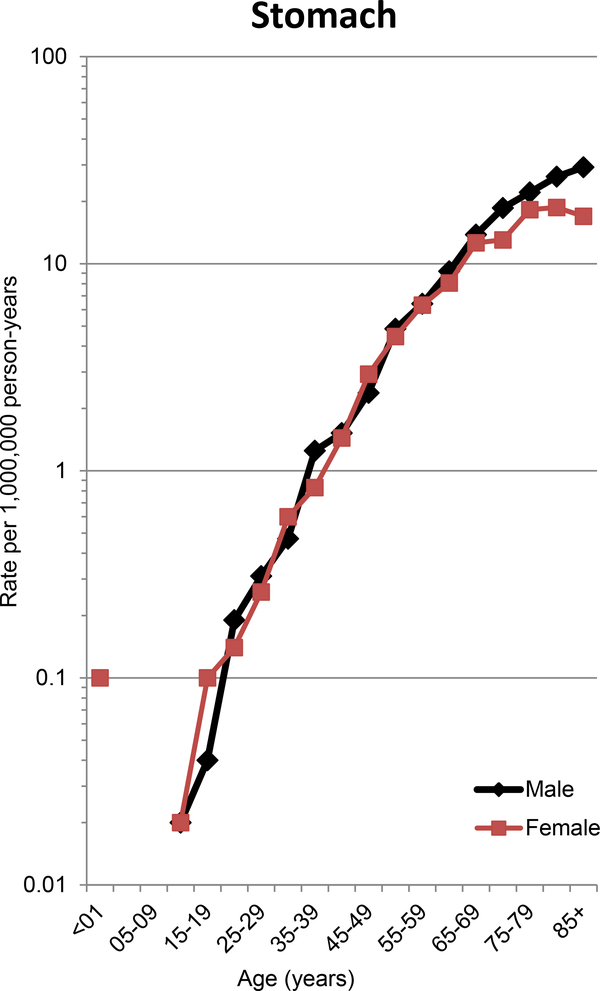
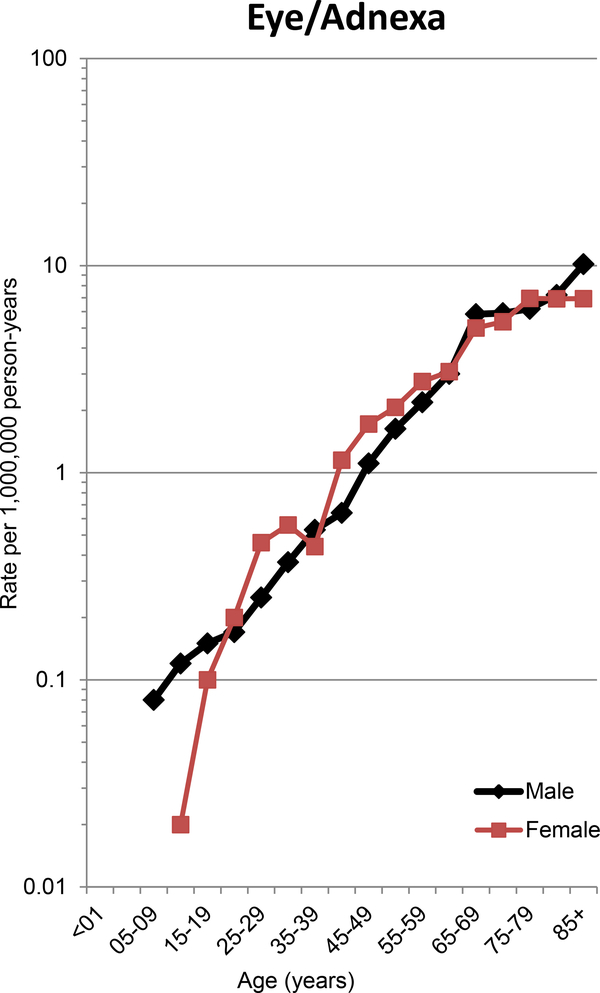
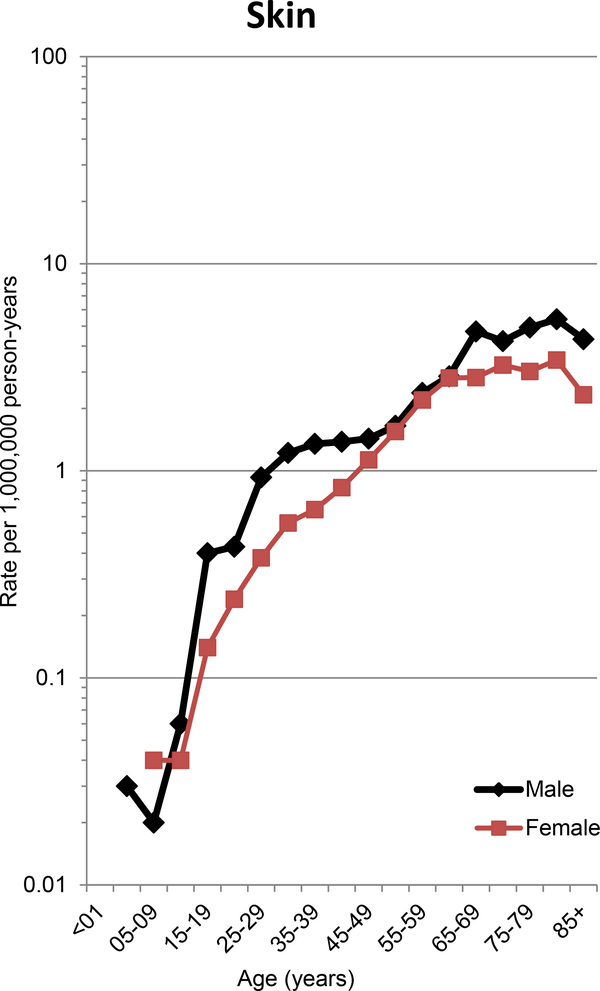
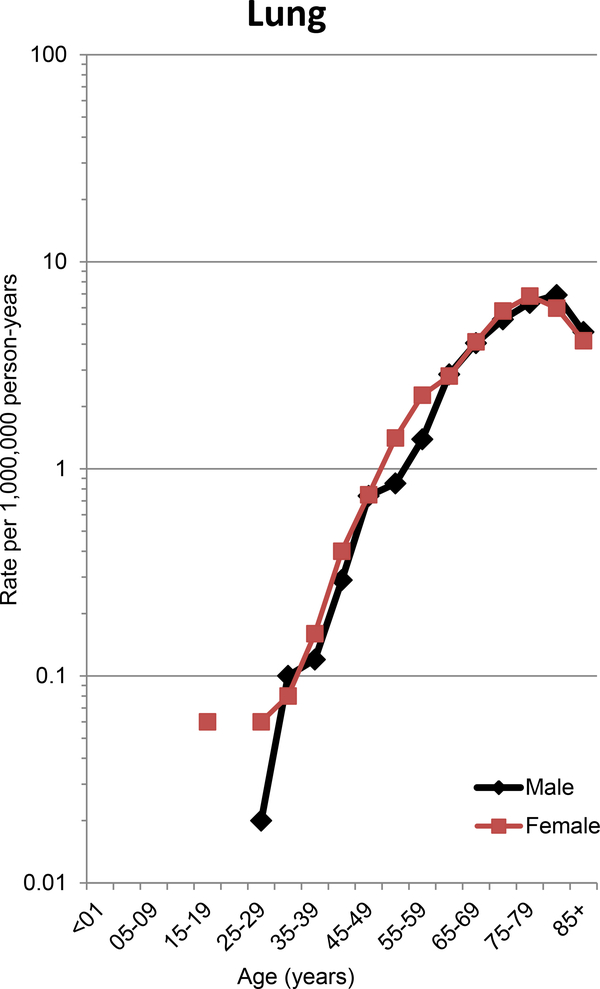
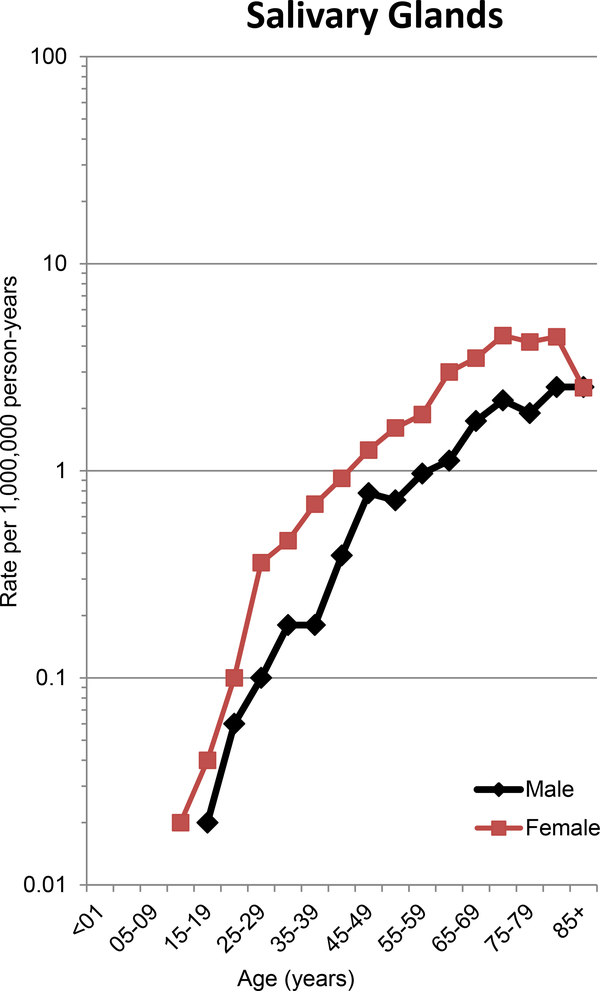
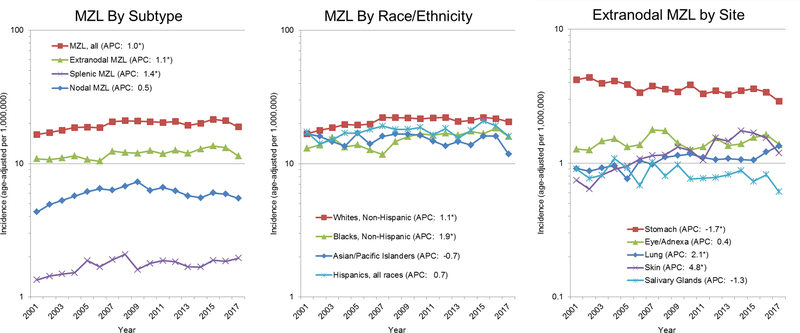
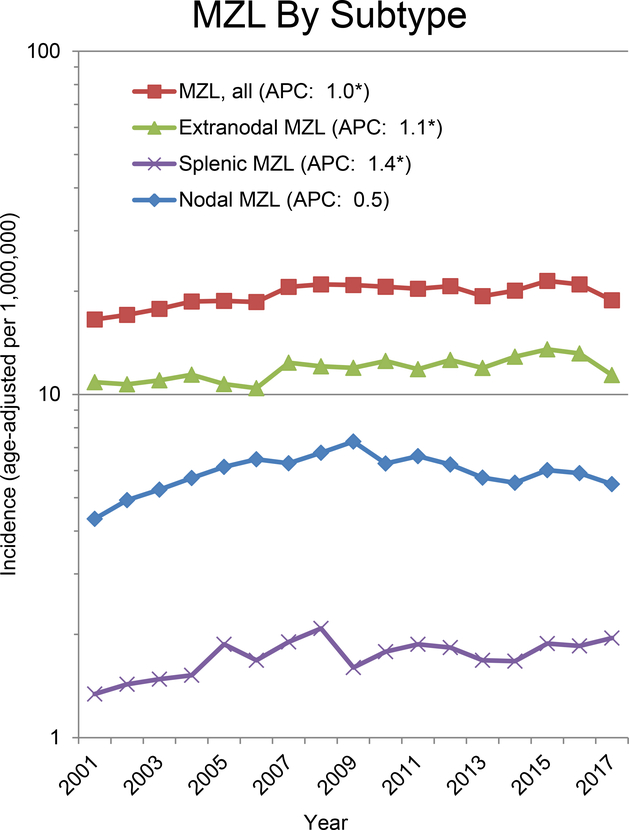
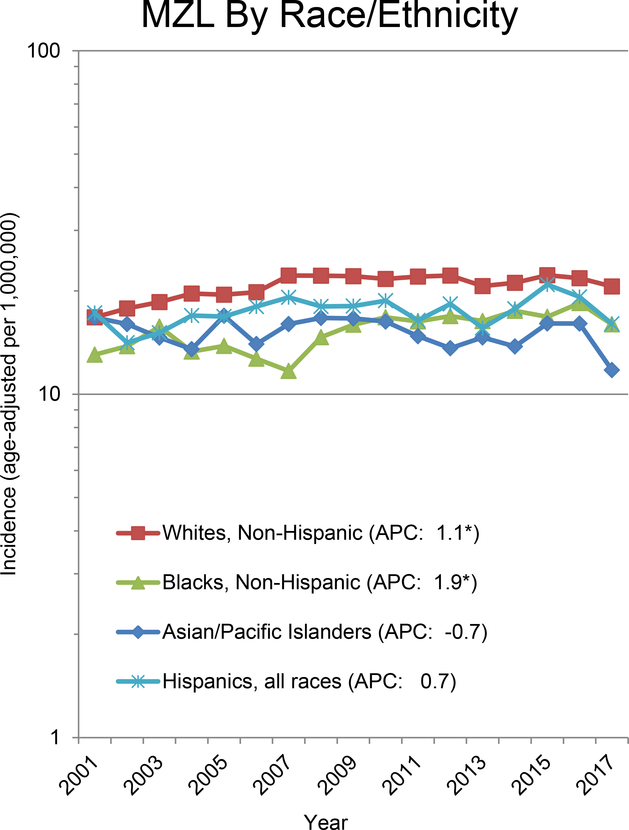
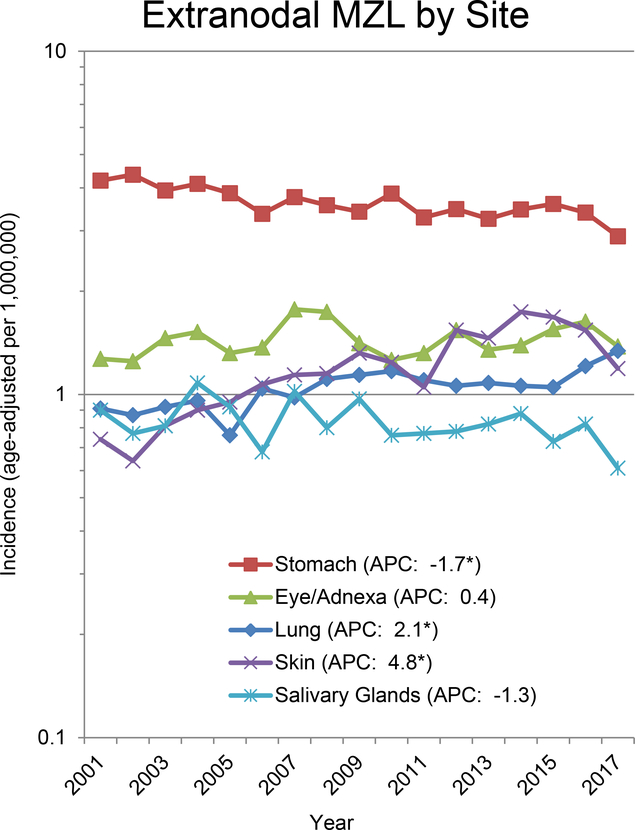
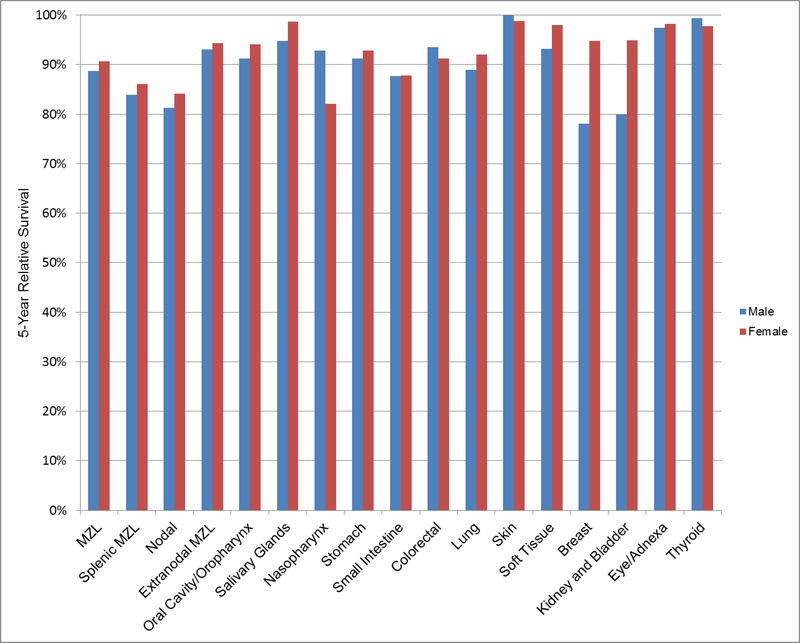
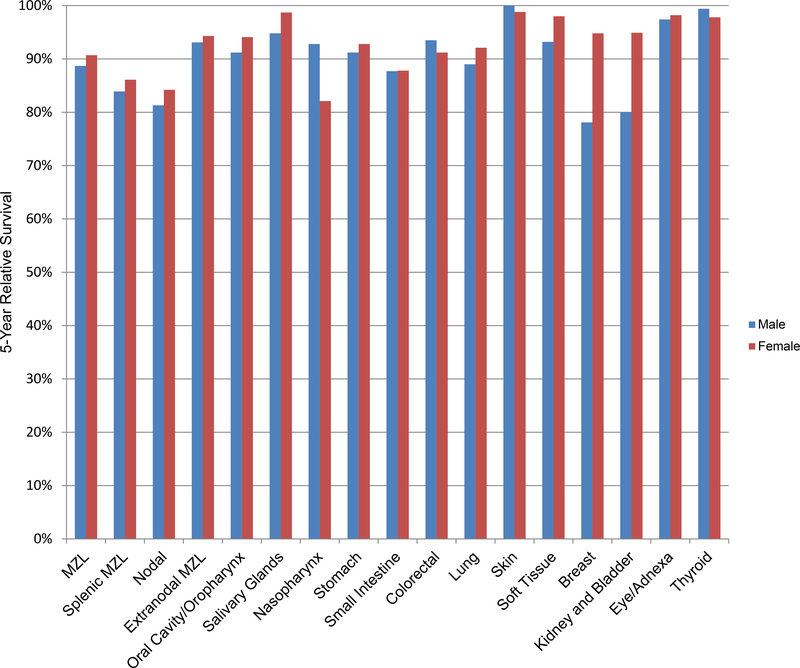
In 2016 there were an estimated 7,460 newly diagnosed patients with marginal zone lymphoma (MZL) in the US, which comprised 7% of all mature non-Hodgkin lymphomas (NHL). Based on data from the US SEER-18 program from 2001-2017, the age-standardized incidence rate for MZL was 19.6 per 1,000,000 person-years; 9% of MZL cases were splenic MZL (SMZL), 30% nodal MZL (NMZL), and 61% extranodal MZL (EMZL) of mucusa-associated lymphoid tissue (MALT). Incidence rates were slightly higher in men for SMZL and NMZL, but similar for EMZL, and increased steeply with age for all MZL subtypes. The incidence (age-standardized per 1,000,000) of MZL was highest among non-Hispanic whites (20.7), followed by Hispanics of all races (17.6), non-Hispanic blacks (15.4), and Asian/Pacific islanders (15.0). The incidence of MZL increased +1.0% per year in the US from 2001-2017, with increases reported in other countries during this timeframe. The 5-year relative survival rate for MZL in the US was 89.8% and was similar across racial/ethnic groups and by sex; survival rates have been increasing in the US and other countries. Established risk factors for MZL (or MZL subtypes) include family history of NHL, genetic loci in the HLA region, Helicobacter pylori infection (gastric MALT lymphoma), and several autoimmune diseases (Sjögren syndrome, systemic lupus erythematosus and Hashimoto thyroiditis), with strong (but not definitive) evidence for Chlamydia psittaci (ocular adnexal MALT lymphoma), Borrelia burgdorferi (cutaneous MZL), hepatitis C virus, human immunodeficiency virus, and solid organ transplantation. Promising risk factors that require additional study include other infections, other autoimmune conditions, trichloroethylene exposure, certain occupations, hair dye, cigarette smoking, sun exposure (protective), and alcohol use (protective). MZL is a model of an antigen-driven malignancy, where epidemiologic risk factors, tissue-specific factors, and host immune response (including the impact of chronic inflammation and immunosuppression) drive lymphomagenesis with implications for prevention.
Keywords: epidemiology; genetics; incidence; marginal zone lymphoma; risk factors.
Figures
References
-
- Teras LR, DeSantis CE, Cerhan JR, Morton LM, Jemal A, Flowers CR. 2016 US lymphoid malignancy statistics by World Health Organization subtypes. CA Cancer J Clin. 2016;66(6):443–59. - PubMed
-
- Isaacson P, Wright DH. Malignant lymphoma of mucosa-associated lymphoid tissue. A distinctive type of B-cell lymphoma. Cancer. 1983;52(8):1410–6. - PubMed
-
- Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML, et al. A revised European-American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study Group [see comments]. Blood. 1994;84(5):1361–92. - PubMed
-
- Jaffe ES, Harris NL, Stein H, Vardiman JW. World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2001.
-
- Fritz A, Percy C, Jack A, Shanmugaratnam K, Sobin L, Parkin DM, et al. International Classification of Diseases for Oncology: Third Edition. Geneva: World Health Organization; 2000. 240 p.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials