

Textbook process as a composite quality indicator for in-hospital hip fracture care
- PMID: 33829364
- PMCID: PMC8026419
- DOI: 10.1007/s11657-021-00909-6
Textbook process as a composite quality indicator for in-hospital hip fracture care
Abstract
Individual process indicators often do not enable the benchmarking of hospitals and often lack an association with outcomes of care. The composite hip fracture process indicator, textbook process, might be a tool to detect hospital variation and is associated with better outcomes during hospital stay.
Purpose: The aim of this study was to determine hospital variation in quality of hip fracture care using a composite process indicator (textbook process) and to evaluate at patient level whether fulfilment of the textbook process indicator was associated with better outcomes during hospital stay.
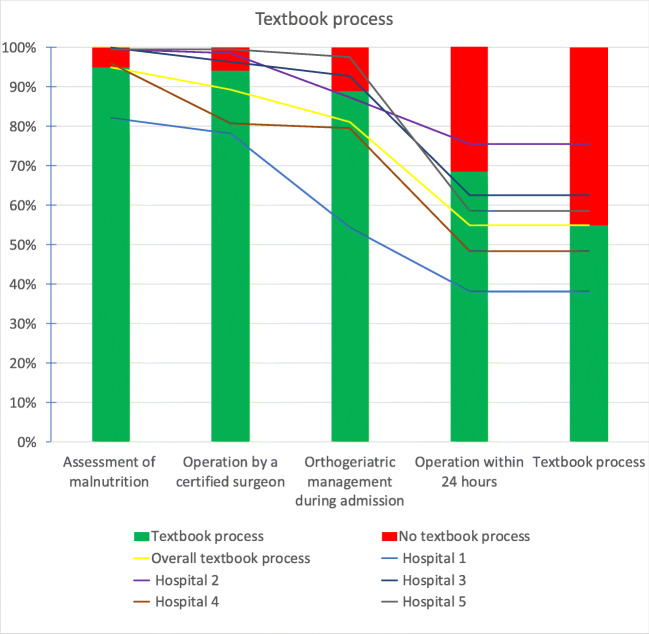
Methods: Hip fracture patients aged 70 and older operated in five hospitals between 1 January 2018 and 31 December 2018 were included. Textbook process for hip fracture care was defined as follows: (1) assessment of malnutrition (2) surgery within 24 h, (3) orthogeriatric management during admission and (4) operation by an orthopaedic trauma certified surgeon. Hospital variation analysis was done by computing an observed/expected ratio (O/E ratio) for textbook process at hospital level. The expected ratios were derived from a multivariable logistic regression analysis including all relevant case-mix variables. The association between textbook process compliance and in-hospital complications and prolonged hospital stay was determined at patient level in a multivariable logistic regression model, with correction for patient, treatment and hospital characteristics. In-hospital complications were anaemia, delirium, pneumonia, urinary tract infection, in-hospital fall, heart failure, renal insufficiency, pulmonary embolism, wound infection and pressure ulcer.
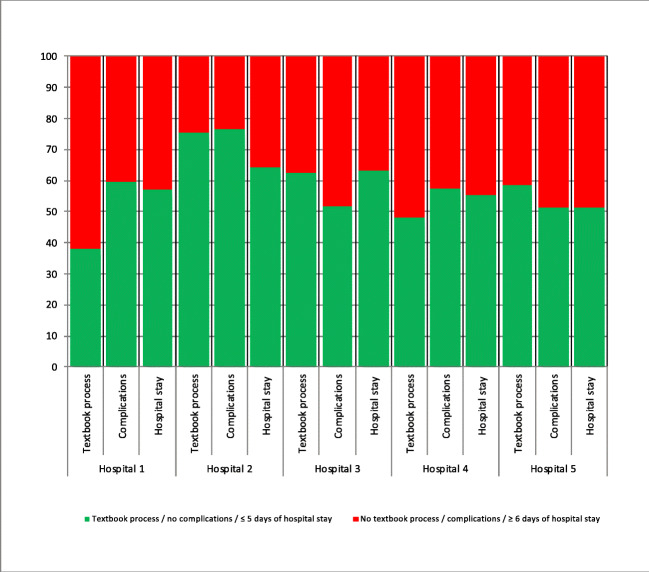
Results: Of the 1371 included patients, 753 (55%) received care according to textbook process. At hospital level, the textbook compliance rates ranged from 38 to 76%. At patient level, textbook process compliance was significantly associated with fewer complications (38% versus 46%) (OR 0.66, 95% CI 0.52-0.84), but not with hospital stay (median length of hospital stay was 5 days in both groups) (OR 1.01, 95% CI 0.78-1.30).
Conclusion: The textbook process indicator for hip fracture care might be a tool to detect hospital variation. At patient level, this quality indicator is associated with fewer complications during hospital stay.
Keywords: Audit; Hip fracture; Quality of care; Textbook process.
Conflict of interest statement
None.
Figures
Similar articles
-
Effect of the Dutch Hip Fracture Audit implementation on mortality, length of hospital stay and time until surgery in elderly hip fracture patients; a multi-center cohort study.Injury. 2020 Apr;51(4):1038-1044. doi: 10.1016/j.injury.2020.02.084. Epub 2020 Feb 19. Injury. 2020. PMID: 32115205
-
Are Case Volume and Facility Complexity Level Associated With Postoperative Complications After Hip Fracture Surgery in the Veterans Affairs Healthcare System?Clin Orthop Relat Res. 2019 Jan;477(1):177-190. doi: 10.1097/CORR.0000000000000460. Clin Orthop Relat Res. 2019. PMID: 30179946 Free PMC article.
-
Impact of orthogeriatric management on the average length of stay of patients aged over seventy five years admitted to hospital after hip fractures.Int Orthop. 2021 Jun;45(6):1431-1438. doi: 10.1007/s00264-020-04908-z. Epub 2021 Jan 4. Int Orthop. 2021. PMID: 33398484
-
Orthogeriatric Management: Improvements in Outcomes during Hospital Admission Due to Hip Fracture.Int J Environ Res Public Health. 2021 Mar 16;18(6):3049. doi: 10.3390/ijerph18063049. Int J Environ Res Public Health. 2021. PMID: 33809573 Free PMC article. Review.
-
Quality indicators of hip fracture management. A systematic review.Tunis Med. 2020 Dec;98(12):913-925. Tunis Med. 2020. PMID: 33479993
Cited by
-
Poor prognosis and risk factors of nonoperative treatment hip fracture patients with end-stage renal disease.Medicine (Baltimore). 2024 Jan 19;103(3):e36446. doi: 10.1097/MD.0000000000036446. Medicine (Baltimore). 2024. PMID: 38241579 Free PMC article.
-
Which performance indicators are used globally for evaluating healthcare in patients with a hip fracture? : a mixed methods systematic review.Bone Jt Open. 2025 Mar 6;6(3):275-290. doi: 10.1302/2633-1462.63.BJO-2024-0104.R1. Bone Jt Open. 2025. PMID: 40043739 Free PMC article.
References
-
- Kolfschoten NE, Gooiker GA, Bastiaannet E, van Leersum NJ, van de Velde CJ, Eddes EH, et al. Combining process indicators to evaluate quality of care for surgical patients with colorectal cancer: are scores consistent with short-term outcome? BMJ Qual Saf. 2012;21(6):481–489. doi: 10.1136/bmjqs-2011-000439. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
