

Diabetes and Frailty: An Expert Consensus Statement on the Management of Older Adults with Type 2 Diabetes
- PMID: 33830409
- PMCID: PMC8099963
- DOI: 10.1007/s13300-021-01035-9
Diabetes and Frailty: An Expert Consensus Statement on the Management of Older Adults with Type 2 Diabetes
Abstract
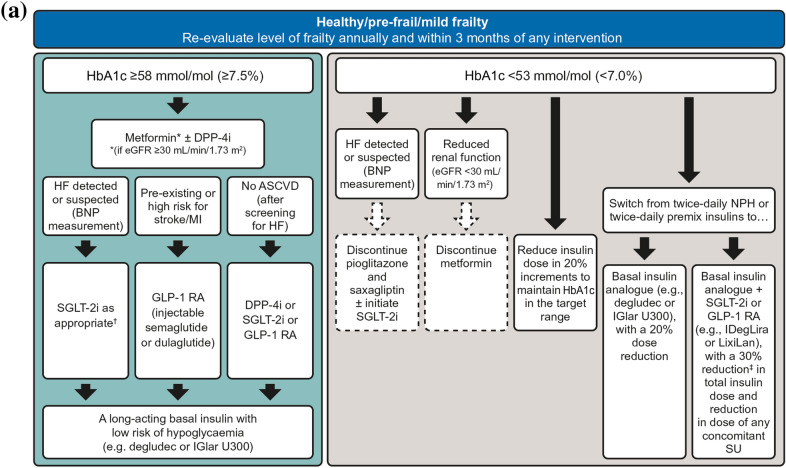
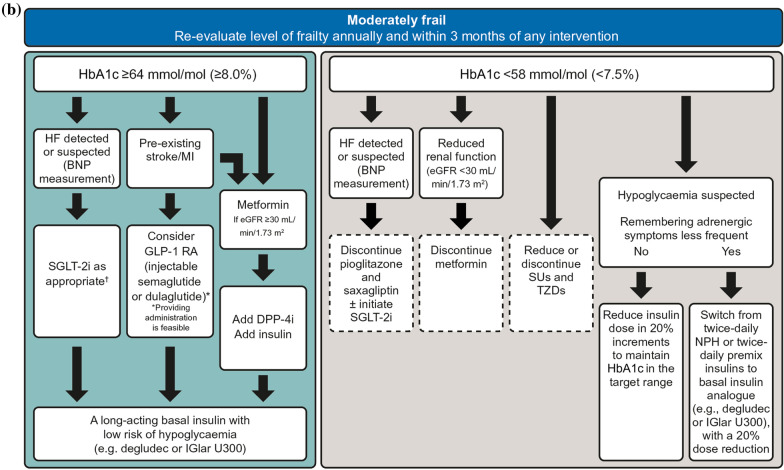
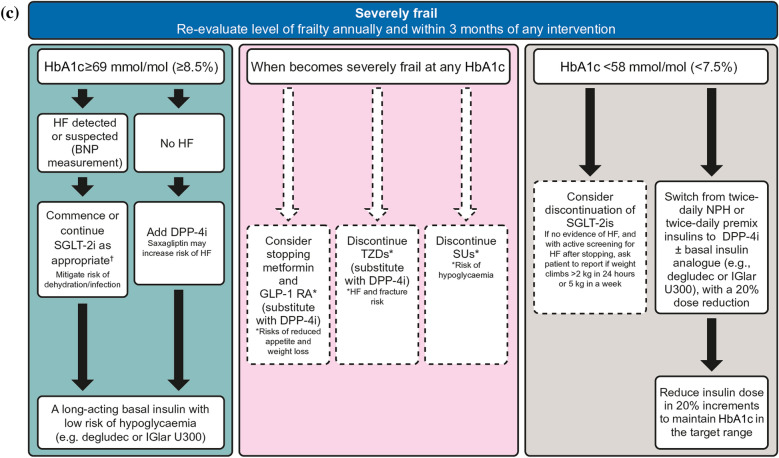
Prognosis and appropriate treatment goals for older adults with diabetes vary greatly according to frailty. It is now recognised that changes may be needed to diabetes management in some older people. Whilst there is clear guidance on the evaluation of frailty and subsequent target setting for people living with frailty, there remains a lack of formal guidance for healthcare professionals in how to achieve these targets. The management of older adults with type 2 diabetes is complicated by comorbidities, shortened life expectancy and exaggerated consequences of adverse effects from treatment. In particular, older adults are more prone to hypoglycaemia and are more vulnerable to its consequences, including falls, fractures, hospitalisation, cardiovascular events and all-cause mortality. Thus, assessment of frailty should be a routine component of a diabetes review for all older adults, and glycaemic targets and therapeutic choices should be modified accordingly. Evidence suggests that over-treatment of older adults with type 2 diabetes is common, with many having had their regimens intensified over preceding years when they were in better health, or during more recent acute hospital admissions when their blood glucose levels might have been atypically high, and nutritional intake may vary. In addition, assistance in taking medications, as often occurs in later life following implementation of community care strategies or admittance to a care home, may dramatically improve treatment adherence, leading to a fall in glycated haemoglobin (HbA1c) levels. As a person with diabetes gets older, simplification, switching or de-escalation of the therapeutic regimen may be necessary, depending on their level of frailty and HbA1c levels. Consideration should be given, in particular, to de-escalation of therapies that may induce hypoglycaemia, such as sulphonylureas and shorter-acting insulins. We discuss the use of available glucose-lowering therapies in older adults and recommend simple glycaemic management algorithms according to their level of frailty.
Keywords: Elderly; Frailty; Treatment choices; Type 2 diabetes.
Figures
References
-
- Strain WD, Hope SV, Green A, Kar P, Valabhji J, Sinclair AJ. Type 2 diabetes mellitus in older people: a brief statement of key principles of modern day management including the assessment of frailty. A national collaborative stakeholder initiative. Diabet Med. 2018;35:838–845. - PubMed
-
- International Diabetes Federation. Global guideline for managing older people with type 2 diabetes. 2013. https://www.idf.org/e-library/guidelines/78-global-guideline-for-managin.... Accessed 14 Oct 2020.
-
- Sinclair AJ, Abdelhafiz A, Dunning T, et al. An international position statement on the management of frailty in diabetes mellitus: summary of recommendations 2017. J Frailty Aging. 2018;7:10–20. - PubMed
-
- Hambling CE, Khunti K, Cos X, et al. Factors influencing safe glucose-lowering in older adults with type 2 diabetes: a PeRsOn-centred ApproaCh To IndiVidualisEd (PROACTIVE) Glycemic Goals for older people: a position statement of Primary Care Diabetes Europe. Prim Care Diabetes. 2019;13:330–352. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
