

Understanding Active Surveillance for Prostate Cancer
- PMID: 33830822
- PMCID: PMC9810129
- DOI: 10.1200/OP.20.00929
Understanding Active Surveillance for Prostate Cancer
Abstract
Purpose: To assess how active surveillance for prostate cancer is apportioned across specialties and how testing patterns and transition to treatment vary by specialty.
Methods: We used a 20% national sample of Medicare claims to identify men diagnosed with prostate cancer from 2010 through 2016 initiating surveillance (N = 13,048). Patients were assigned to the physician responsible for the bulk of surveillance care based on billing patterns. Freedom from treatment was assessed by specialty of the responsible physician (urology, radiation oncology, medical oncology, and primary care). Multinomial logistic regression models were used to examine associations between specialty and treatment patterns.
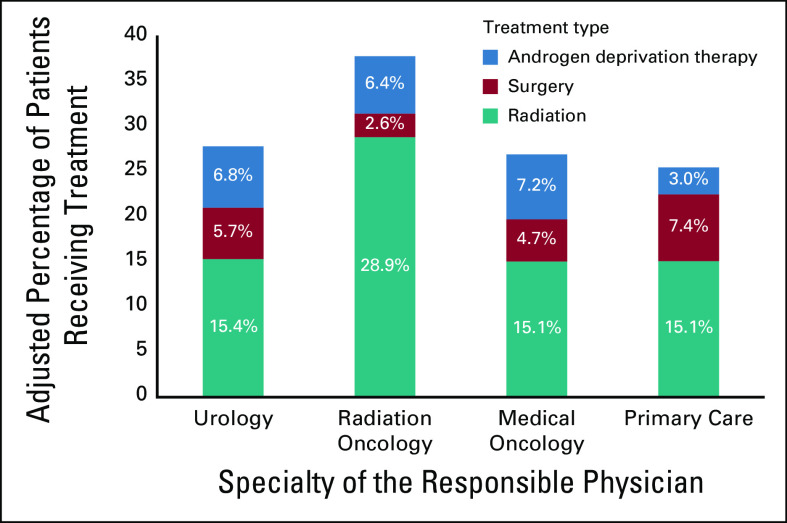
Results: Urologists were responsible for surveillance in 93.7% of patients in 2010 and 96.2% of patients in 2016 (P for trend = .01). Testing patterns varied by specialty. For example, patients of medical oncologists had more frequent prostate-specific antigen testing compared with patients of urologists (1.85 v 2.39 tests per year, respectively; P < .01). Three years after diagnosis, a significantly smaller proportion of patients managed by radiation oncologists (64.3%) remained on surveillance compared with patients managed by other physicians (75.8%-79.5%; P < .01). Although radiation was the most common treatment among all men who transitioned to treatment, a disproportionate percentage of patients followed by radiation oncologists (28.9%) ultimately underwent radiation compared with patients followed by other physicians (15.1%-15.4%; P < .01).
Conclusion: Nontrivial percentages of patients on active surveillance are managed by physicians outside of urology. Given the interspecialty variations observed, efforts to strengthen the evidence underlying surveillance pathways and to engage other specialties in guideline development are needed.
Conflict of interest statement
Figures



Comment in
-
Socioeconomic Factors, Urological Epidemiology and Practice Patterns.J Urol. 2022 Jun;207(6):1337-1338. doi: 10.1097/JU.0000000000002660. Epub 2022 Mar 23. J Urol. 2022. PMID: 35319263 No abstract available.
References
-
- NCI : SEER cancer stat facts: Prostate cancer. 2017. https://seer.cancer.gov/statfacts/html/prost.html
-
- Klotz L, Zhang L, Lam A, et al. : Clinical results of long-term follow-up of a large, active surveillance cohort with localized prostate cancer. J Clin Oncol 28:126-131, 2010 - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, et al. : 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 375:1415-1424, 2016 - PubMed
-
- Klotz L, Vesprini D, Sethukavalan P, et al. : Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol 33:272-277, 2015 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
