

Lead aVR predicts early revascularization but not long-term events in patients referred for stress electrocardiography
- PMID: 33831085
- PMCID: PMC8032194
- DOI: 10.1371/journal.pone.0249779
Lead aVR predicts early revascularization but not long-term events in patients referred for stress electrocardiography
Abstract
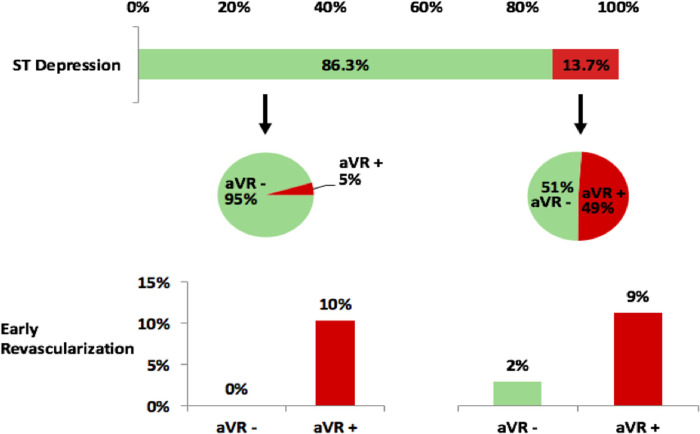
Background: Exercise stress electrocardiography (ExECG) is recommended as a first-line tool to assess ischemia, but standard ST-analysis has limited diagnostic accuracy. ST elevation in lead aVR has been associated with left main and LAD disease in the population undergoing coronary angiography but has not been studied in the general population undergoing stress testing for the initial evaluation of CAD without coronary angiography. We sought to determine the predictive value of lead aVR elevation for ischemia, early revascularization, and subsequent cardiac events in consecutive patients undergoing ExECG.
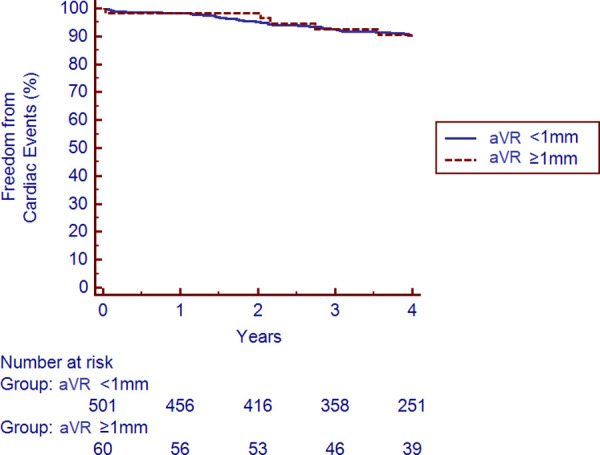
Methods and results: The study cohort included 641 subjects referred for ExECG who were dichotomized by presence or absence of aVR elevation ≥1mm and compared for prevalence and predictors of ischemia and a composite of cardiac death, nonfatal myocardial infarction, and late revascularization. The cohort had a median age of 57 and 57% were male. The prevalence of aVR elevation was 11.5%. The prevalence of significant ischemia on patients who received imaging was significantly higher with aVR elevation (14.3% vs 2.3%, p<0.001). Early revascularization occurred in 10.9% with vs 0.2% without aVR elevation, p<0.001. No subjects without aVR elevation or ST-depression underwent early revascularization. However, cardiac event rates were similar over a median 4.0 years of follow-up with and without aVR elevation (2.8% vs. 2.6%, p = 0.80). aVR elevation did not predict long-term cardiac events by Kaplan-Meier survival analysis (p = 0.94) or Cox proportional hazards modeling (p = 0.35).
Conclusions: aVR elevation during ExECG predicts ischemia on imaging and early revascularization but not long-term outcomes and could serve as a useful adjunct to standard ST-analysis and potentially reduce the need for concurrent imaging.
Conflict of interest statement
Dr. Bourque performs consulting with Pfizer Inc. and General Electric. He has investment interest with Locus Health. This does not alter our adherence to PLOS ONE policies on sharing data and materials. The other authors have nothing to disclose.
Figures



References
-
- Gibbons RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, Froelicher VF, et al.. ACC/AHA 2002 guideline update for exercise testing: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). J Am Coll Cardiol. 2002;40: 1531–1540. 10.1016/s0735-1097(02)02164-2 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
