

Broad and potent neutralizing human antibodies to tick-borne flaviviruses protect mice from disease
- PMID: 33831141
- PMCID: PMC8040517
- DOI: 10.1084/jem.20210236
Broad and potent neutralizing human antibodies to tick-borne flaviviruses protect mice from disease
Abstract
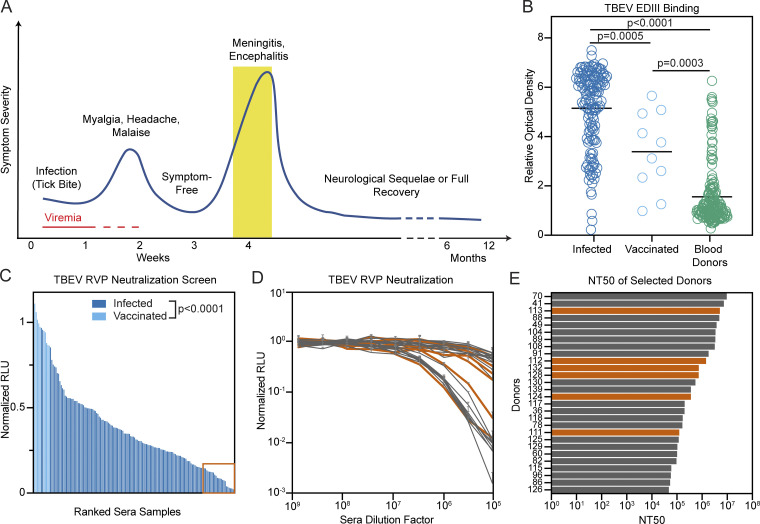
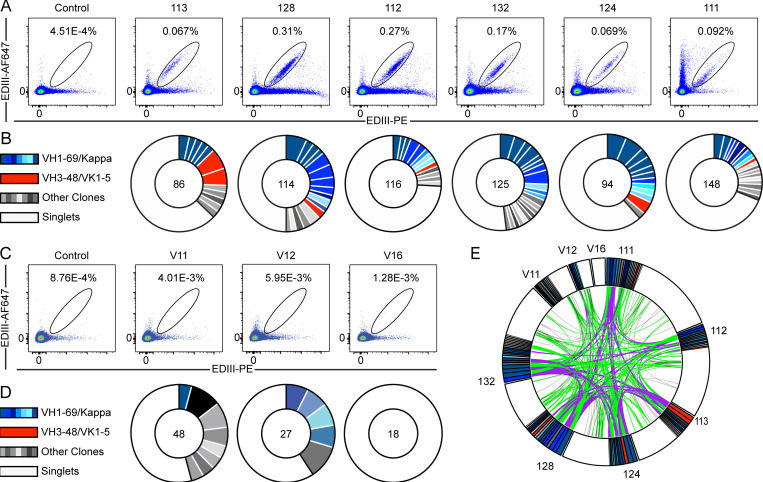
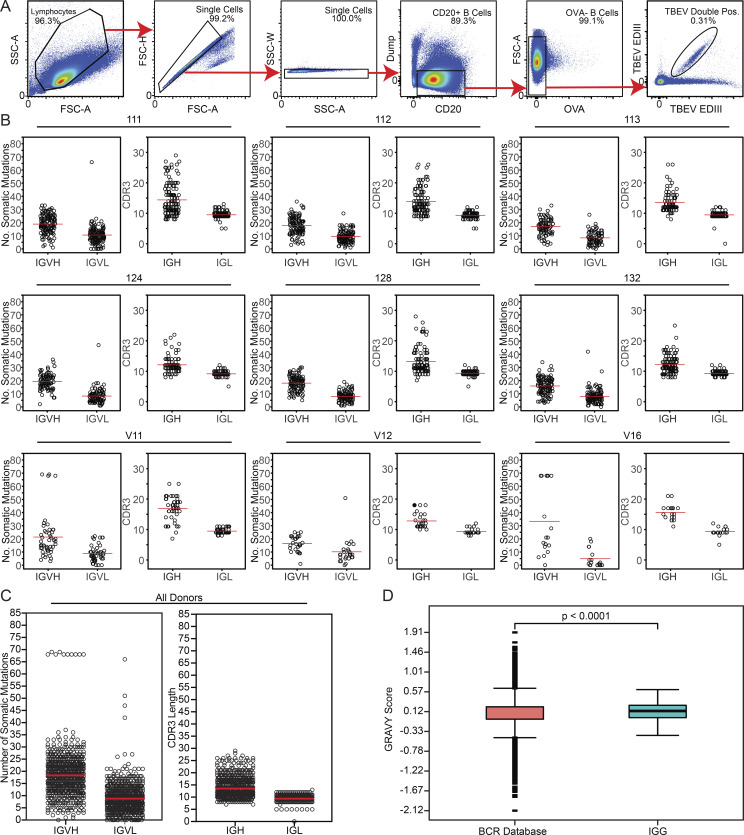
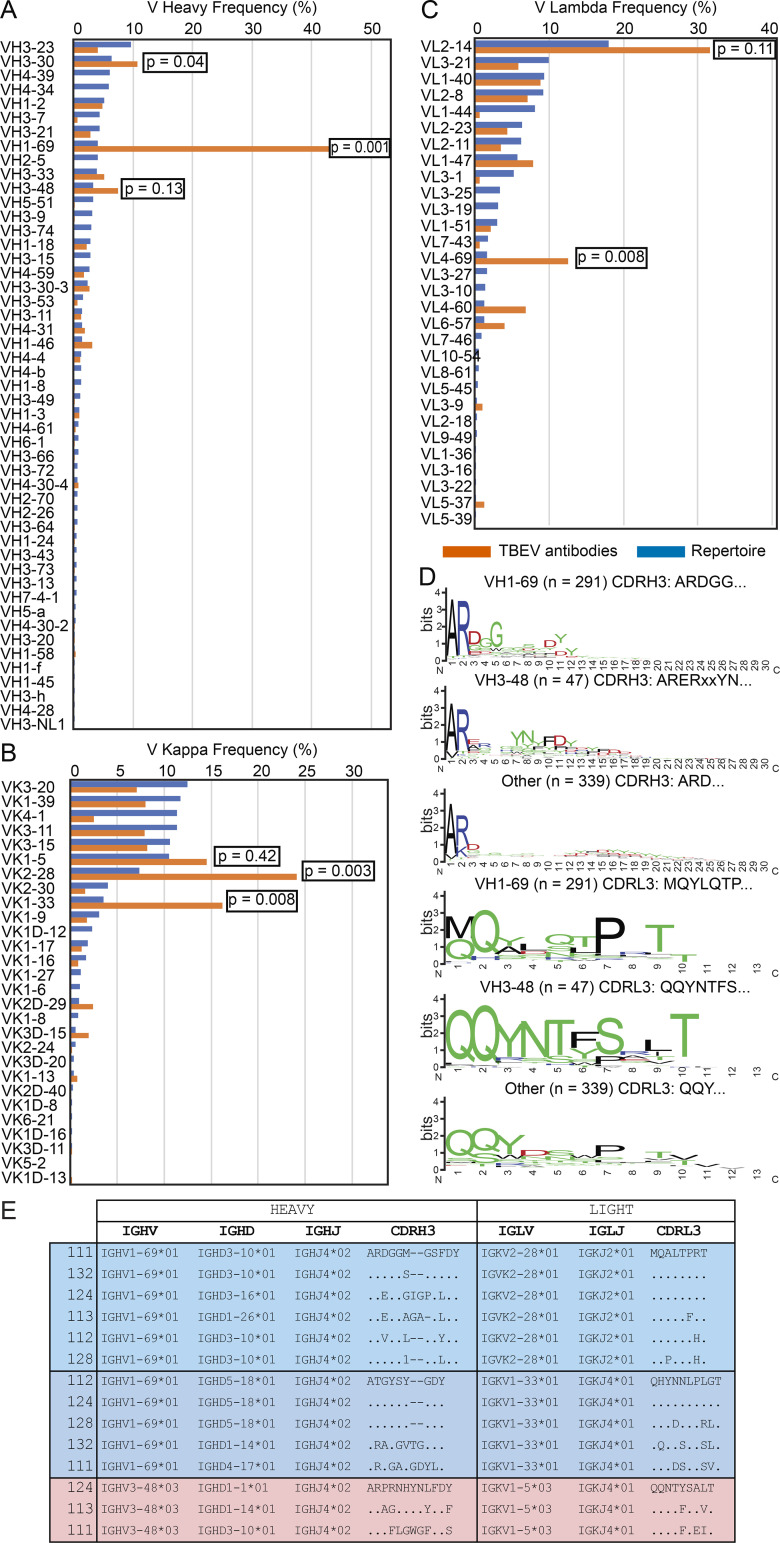
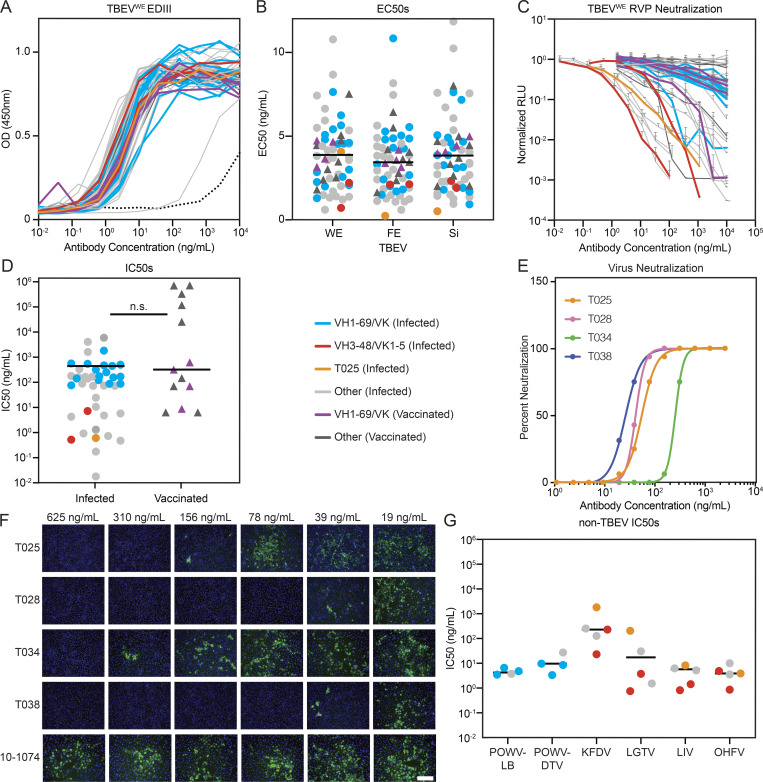
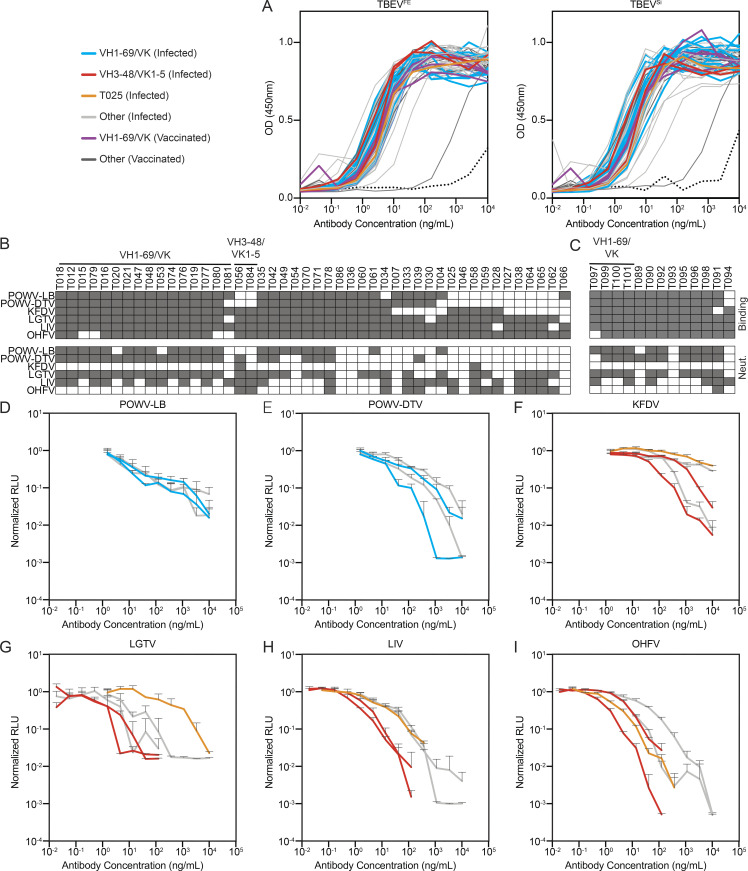
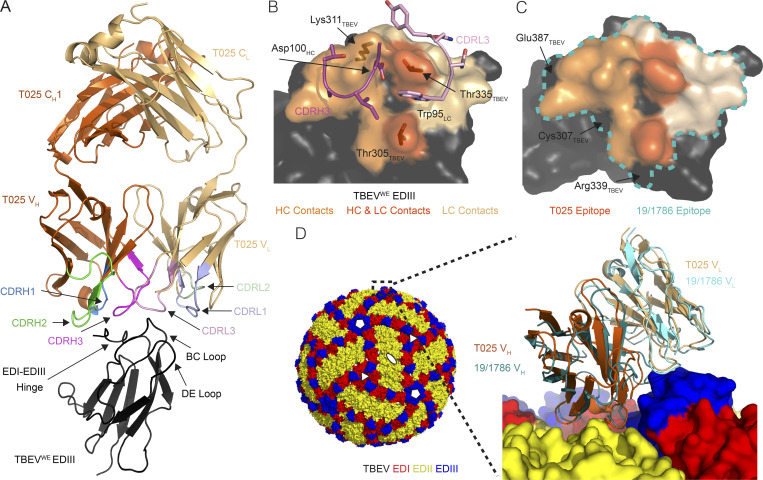
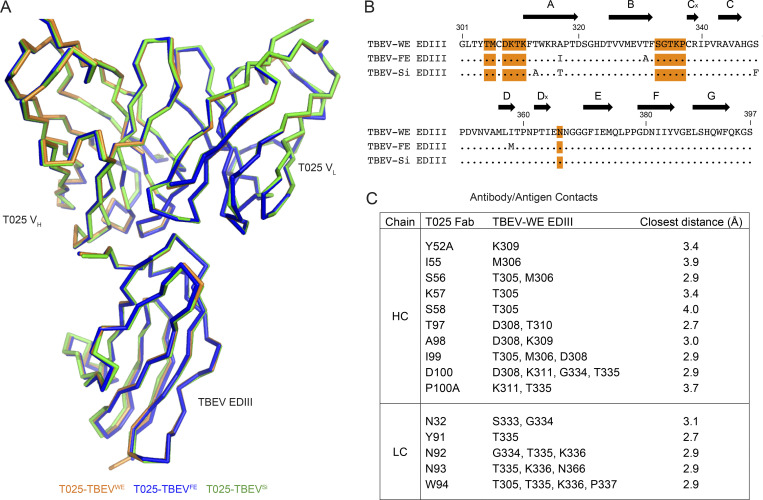
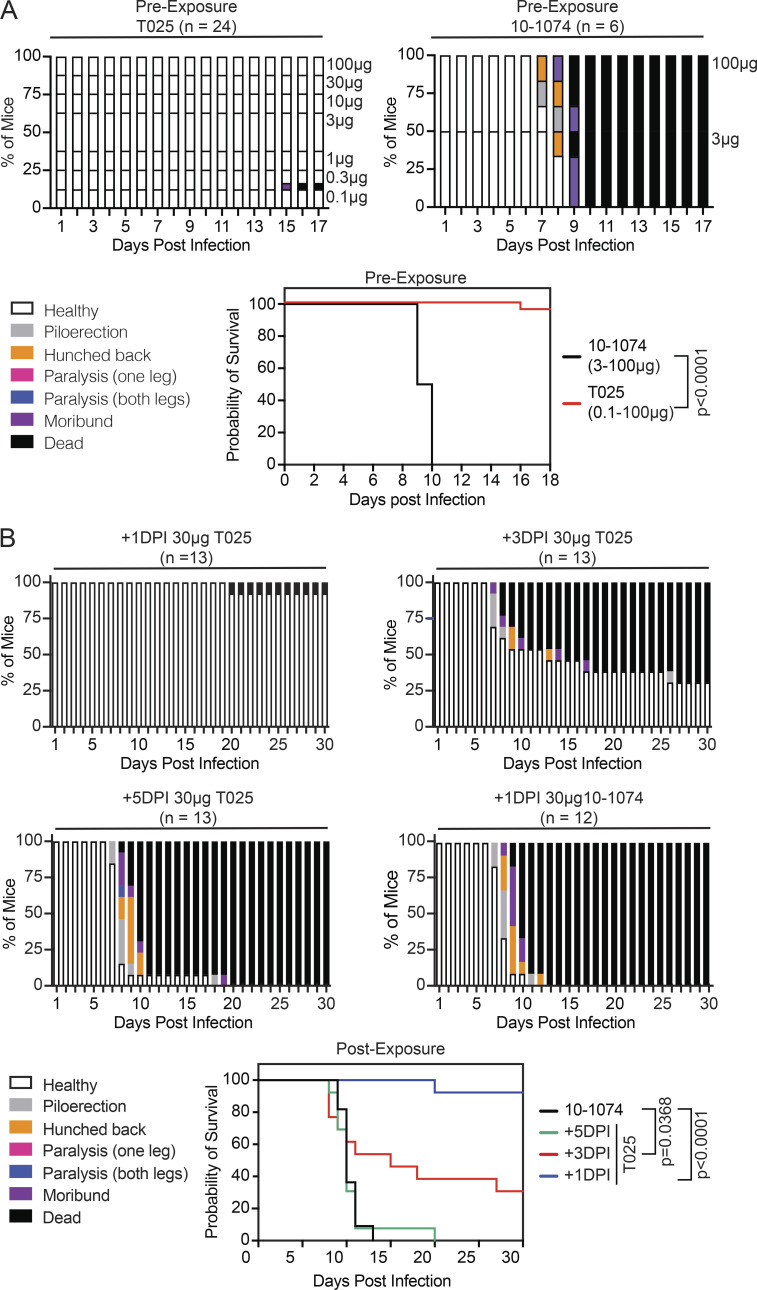
Tick-borne encephalitis virus (TBEV) is an emerging human pathogen that causes potentially fatal disease with no specific treatment. Mouse monoclonal antibodies are protective against TBEV, but little is known about the human antibody response to infection. Here, we report on the human neutralizing antibody response to TBEV in a cohort of infected and vaccinated individuals. Expanded clones of memory B cells expressed closely related anti-envelope domain III (EDIII) antibodies in both groups of volunteers. However, the most potent neutralizing antibodies, with IC50s below 1 ng/ml, were found only in individuals who recovered from natural infection. These antibodies also neutralized other tick-borne flaviviruses, including Langat, louping ill, Omsk hemorrhagic fever, Kyasanur forest disease, and Powassan viruses. Structural analysis revealed a conserved epitope near the lateral ridge of EDIII adjoining the EDI-EDIII hinge region. Prophylactic or early therapeutic antibody administration was effective at low doses in mice that were lethally infected with TBEV.
© 2021 Agudelo et al.
Conflict of interest statement
Disclosures: M. Agudelo, D.F. Robbiani, and M.C. Nussenzweig reported a patent to Broadly Neutralizing Antibodies to Tick-Borne Encephalitis and Related Viruses (US 63/118,461) pending. M.C. Nussenzweig reported personal fees from Celldex outside the submitted work. Additionally, M.C. Nussenzweig is a Frontier Bioscience SAB member. No other disclosures were reported.
Figures
References
-
- Adams, P.D., Afonine P.V., Bunkóczi G., Chen V.B., Davis I.W., Echols N., Headd J.J., Hung L.W., Kapral G.J., Grosse-Kunstleve R.W., et al. 2010. PHENIX: a comprehensive Python-based system for macromolecular structure solution. Acta Crystallogr. D Biol. Crystallogr. 66:213–221. 10.1107/S0907444909052925 - DOI - PMC - PubMed
-
- Albinsson, B., Vene S., Rombo L., Blomberg J., Lundkvist Å., and Rönnberg B.. 2018. Distinction between serological responses following tick-borne encephalitis virus (TBEV) infection vs vaccination, Sweden 2017. Euro Surveill. 23:17–00838. 10.2807/1560-7917.ES.2018.23.3.17-00838 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
