

Femoral nerve block versus fascia iliaca block for pain control in knee and hip arthroplasties: A meta-analysis
- PMID: 33832151
- PMCID: PMC8036080
- DOI: 10.1097/MD.0000000000025450
Femoral nerve block versus fascia iliaca block for pain control in knee and hip arthroplasties: A meta-analysis
Abstract
Background: This meta-analysis aimed to compare the efficiency of fascia iliaca compartment block (FICB) and femoral nerve block (FNB) for pain management in knee and hip surgeries.
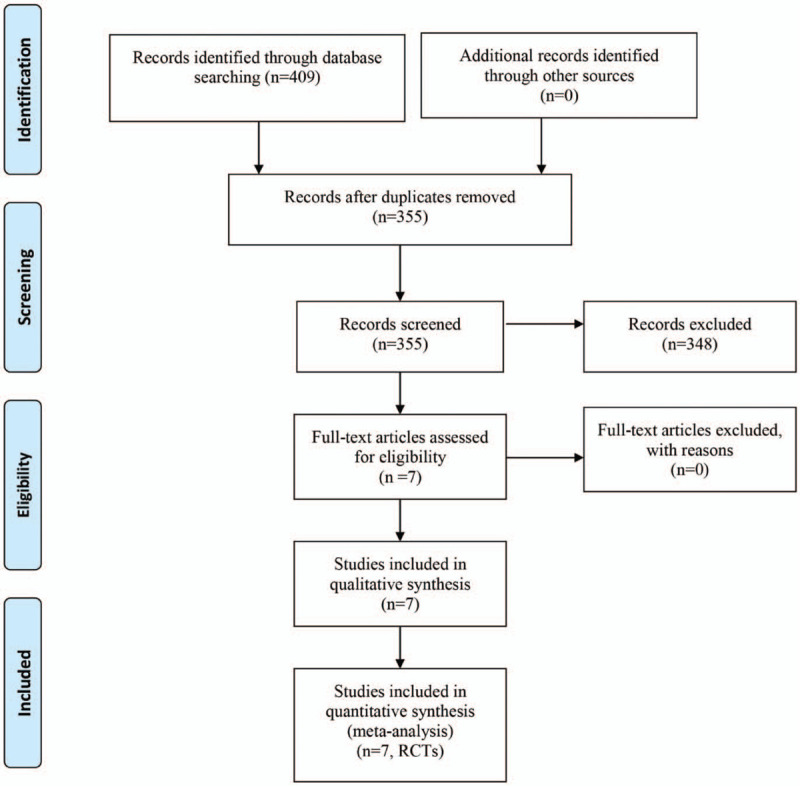
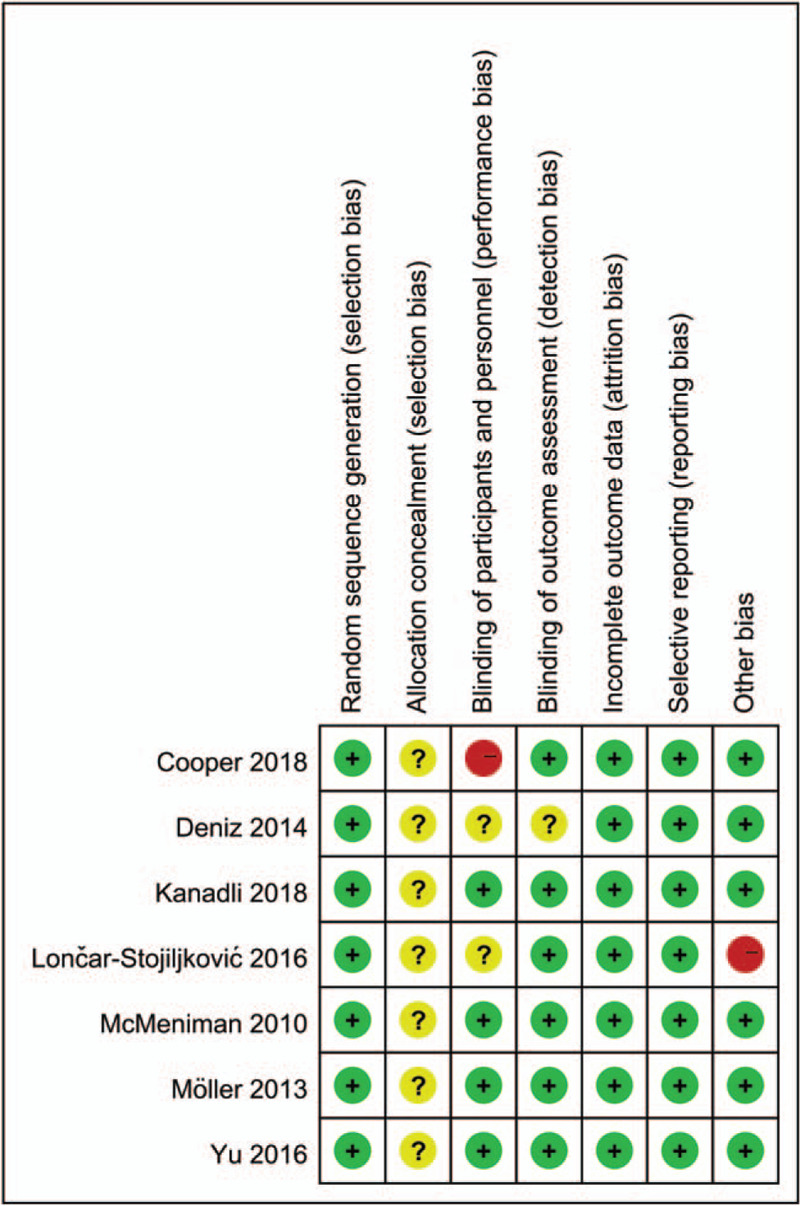
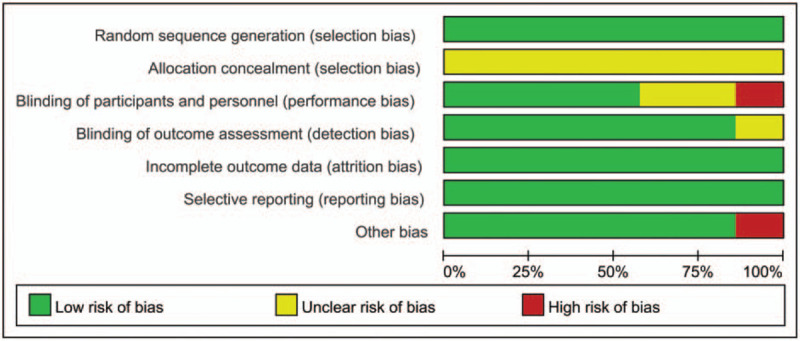
Methods: We searched four electronic databases (Pubmed, Embase, Cochrane library database, Web of Science) from inception to January 2019. Only randomized controlled trials (RCTs) were included. Two review authors independently extracted data for each included study. Primary outcomes were visual analogue scale at 12 hours, 24 hours, 48 hours, total morphine consumption, the length of hospital stay and the occurrence of nausea and vomiting. Standardized mean difference (SMD) or risk ratio (RR) and 95% confidence intervals (CIs) were calculated for continuous outcomes and discontinuous outcomes respectively. We used the Cochrane Risk of Bias tool to assess risk of bias. Stata 12.0 was used for meta-analysis.
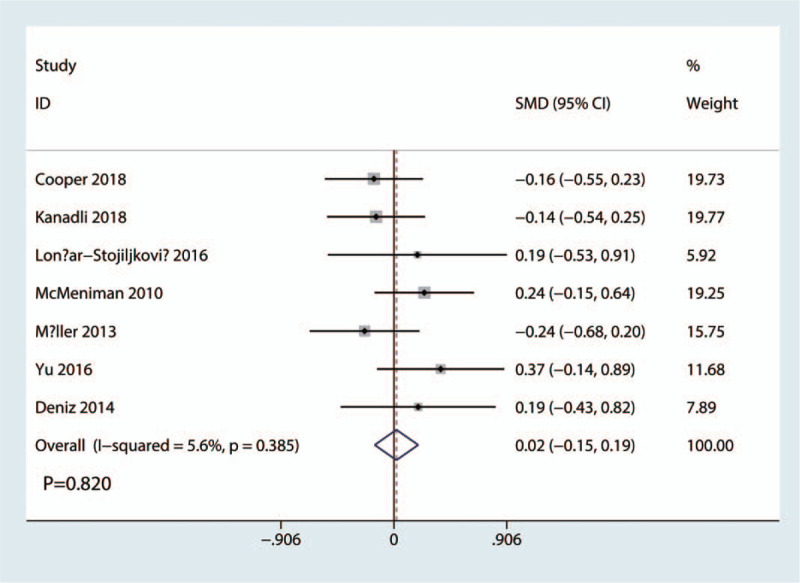
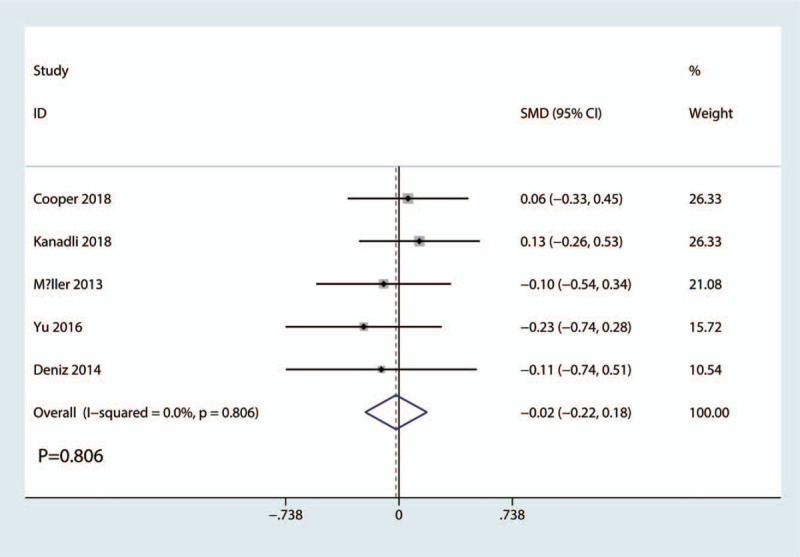
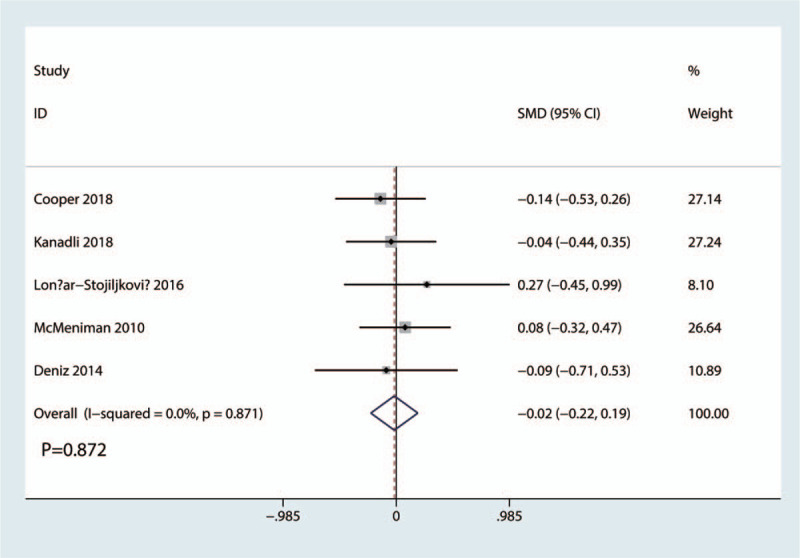
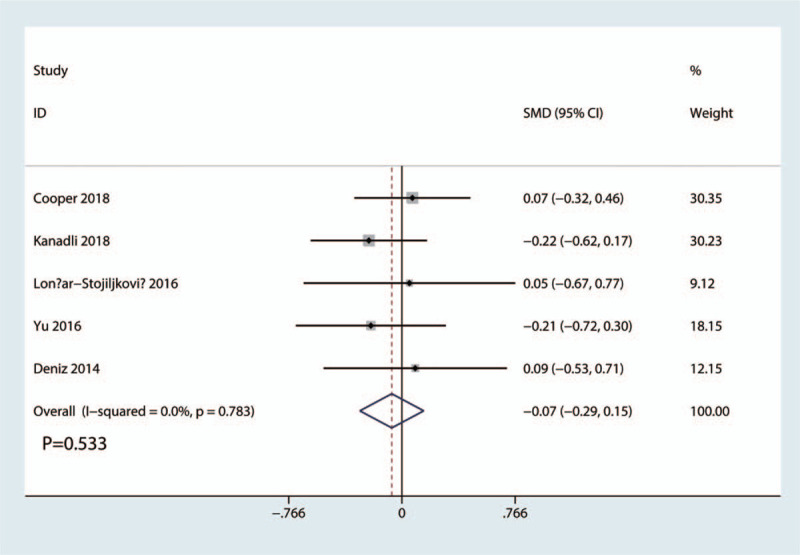
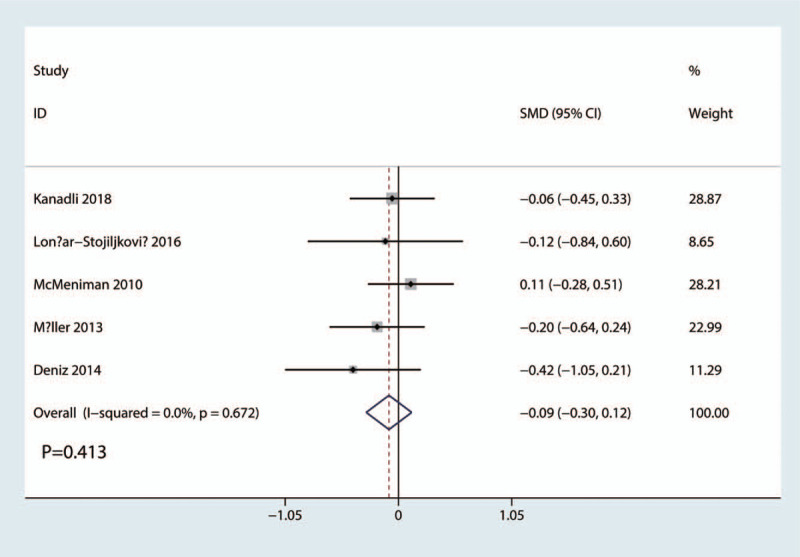
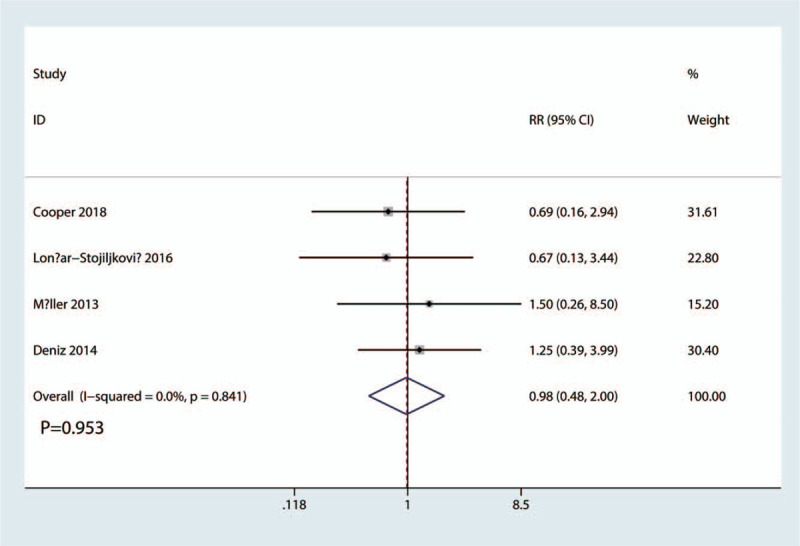
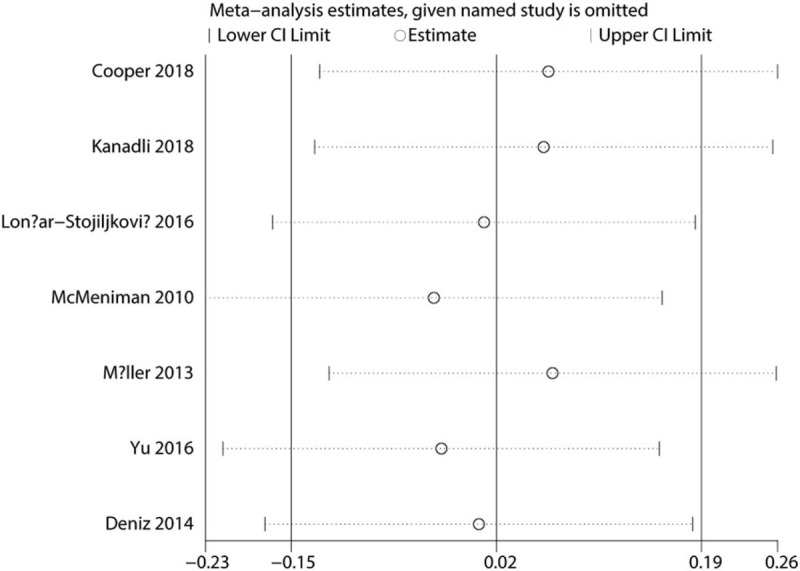
Results: Finally, 7 RCTs involving 508 patients (FICB = 254, FNB = 254) were included in this meta-analysis. Compared with FNB group, FICB has no benefit for visual analogue scale at 12 hours (SMD = 0.02, 95% CI, -0.15 to 0.19; P = .820), 24 hours (SMD = -0.02, 95% CI, -0.22 to 0.18; P = .806), and 48 hours (SMD = -0.02, 95% CI, -0.22 to 0.19; P = .872). No significant differences were found regarding total morphine consumption (SMD = -0.07, 95% CI, -0.29 to 0.15; P = .533). What's more, there was no significant difference between the length of hospital stay and the occurrence of nausea and vomiting (P > .05).
Conclusion: FICB has equivalent pain control and morphine-sparing efficacy when compared with FNB. More high-quality RCTs are needed to identify the optimal drugs and volume of local infiltration protocols.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Gaffney CJ, Pelt CE, Gililland JM, et al. Perioperative pain management in hip and knee arthroplasty. Orthop Clin North Am 2017;48:407–19. - PubMed
-
- Affas F. Local infiltration analgesia in knee and hip arthroplasty efficacy and safety. Scand J Pain 2016;13:59–66. - PubMed
-
- Crumley Aybar BL, Gillespie MJ, Gipson SF, et al. Peripheral nerve blocks causing increased risk for fall and difficulty in ambulation for the hip and knee joint replacement patient. J Perianesth Nurs 2016;31:504–19. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
