

Gastrointestinal symptoms as first remarkable signs of ANCA-associated granulomatosis with polyangiitis: a case report and reviews
- PMID: 33832425
- PMCID: PMC8028736
- DOI: 10.1186/s12876-021-01730-8
Gastrointestinal symptoms as first remarkable signs of ANCA-associated granulomatosis with polyangiitis: a case report and reviews
Abstract
Background: Systemic vasculitis associated with antineutrophil cytoplasmic autoantibodies (ANCA) have an extremely wide variety of symptoms, therefore the fast and proper diagnosis is difficult to establish even for experienced physicians. Gastrointestinal manifestations in ANCA-associated granulomatosis with polyangiitis (GPA) may be present, however, severe, life-threatening complications (such as perforations) are rare.
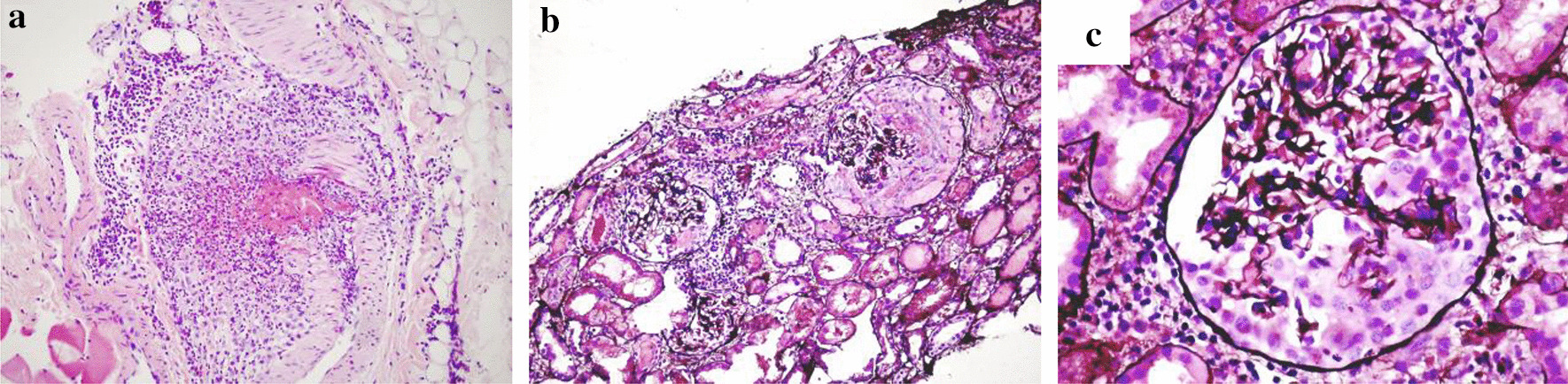
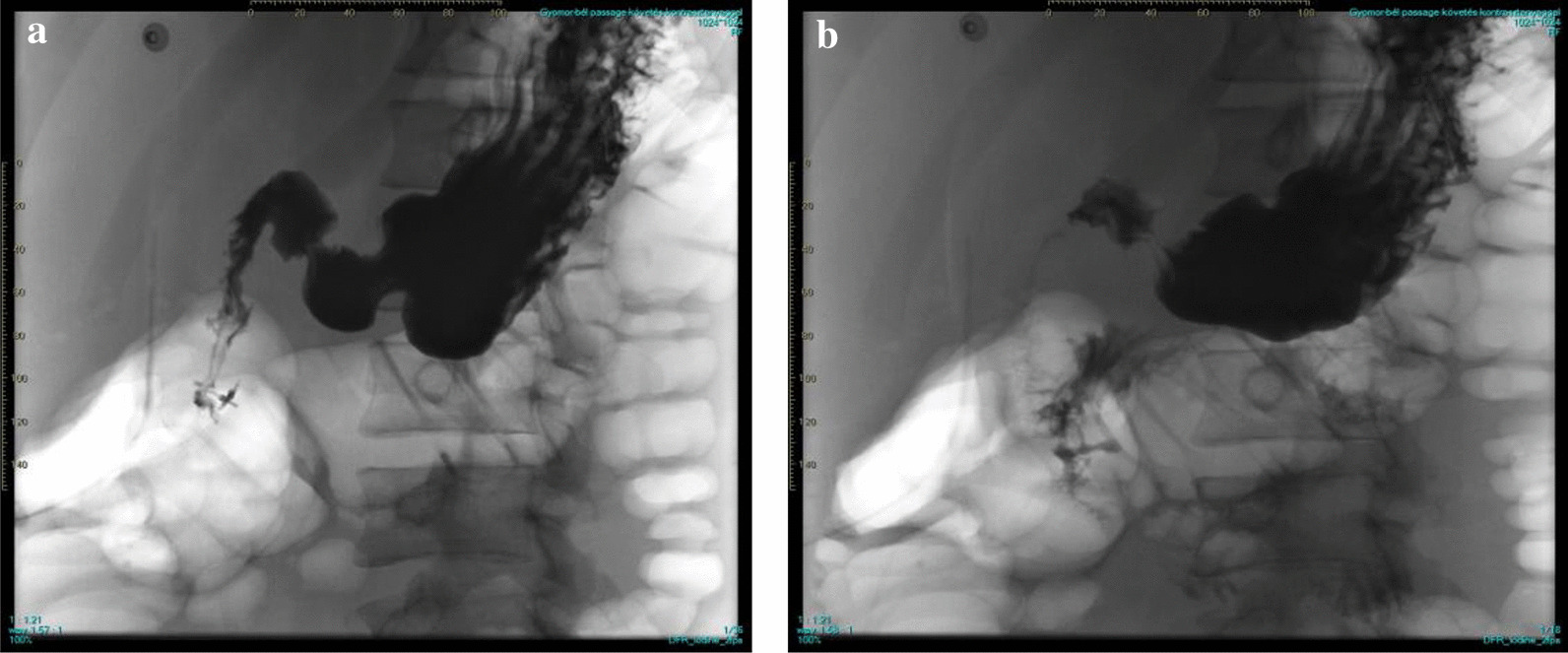
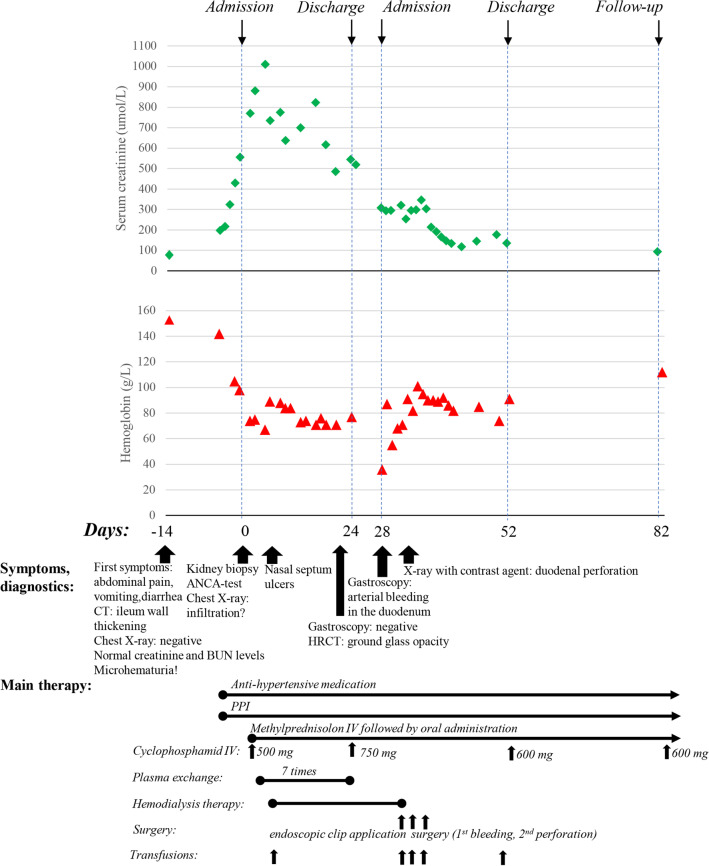
Case presentation: A case of an 18-year-old male patient is presented, where gastrointestinal symptoms (abdominal pain, vomiting, diarrhoea) were the first remarkable signs of GPA. The initial diagnosis of inflammatory bowel disease delayed the administration of proper immunosuppressive therapy, which might have contributed to the rare and life-threatening complication of arterial duodenal bleeding with perforation. Our systematic review of the literature found only a few case reports where gastrointestinal symptoms were the first signs of GPA, however, this entity might be more frequent if physicians would think of this possibility more often.
Conclusions: Gastrointestinal bleeding is a rare but potential lethal complication of vasculitis. Consequently, we recommend investigating the patients diagnosed with GPA for gastrointestinal bleeding during the treatment.
Keywords: Antineutrophil cytoplasmic antibodies; Case report; Gastrointestinal haemorrhage; Granulomatosis with polyangiitis; Systemic vasculitis.
Conflict of interest statement
N.L. declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Á.G.P. declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Falk RJ, Jennette JC. ANCA small-vessel vasculitis. J Am Soc Nephrol. 1997;8(2):314–322. - PubMed
-
- Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, et al. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis. 2007;66(2):222–227. doi: 10.1136/ard.2006.054593. - DOI - PMC - PubMed
-
- Pagnoux C, Mahr A, Cohen P, Guillevin L. Presentation and outcome of gastrointestinal involvement in systemic necrotizing vasculitides: analysis of 62 patients with polyarteritis nodosa, microscopic polyangiitis, Wegener granulomatosis, Churg-Strauss syndrome, or rheumatoid arthritis-associated vasculitis. Medicine (Baltimore) 2005;84(2):115–128. doi: 10.1097/01.md.0000158825.87055.0b. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
