

Reducing prescribing of benzodiazepines in older adults: a comparison of four physician-focused interventions by a medical regulatory authority
- PMID: 33832432
- PMCID: PMC8034172
- DOI: 10.1186/s12875-021-01415-x
Reducing prescribing of benzodiazepines in older adults: a comparison of four physician-focused interventions by a medical regulatory authority
Abstract
Background: The inappropriate and/or high prescribing of benzodiazepine and 'Z' drugs (BDZ +) is a major health concern. The purpose of this study was to determine whether physician or pharmacist led interventions or a simple letter or a personalized prescribing report from a medical regulatory authority (MRA) was the most effective intervention for reducing BDZ + prescribing by physicians to patients 65 years of age or older.
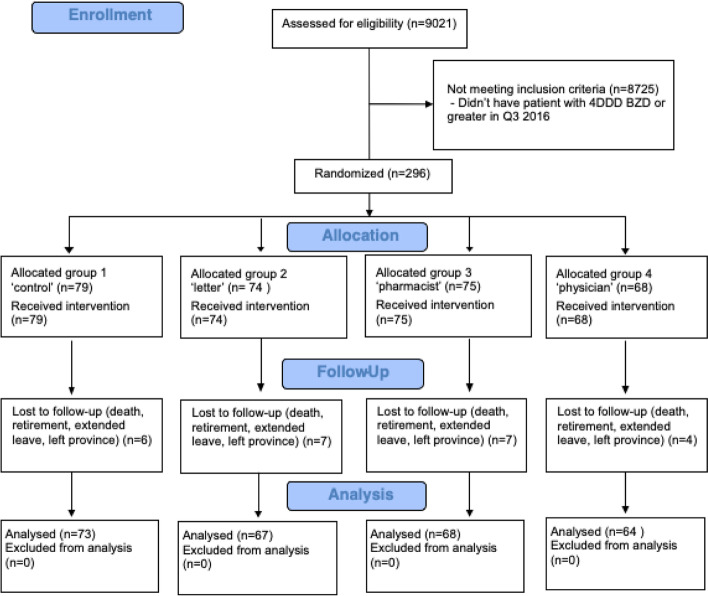
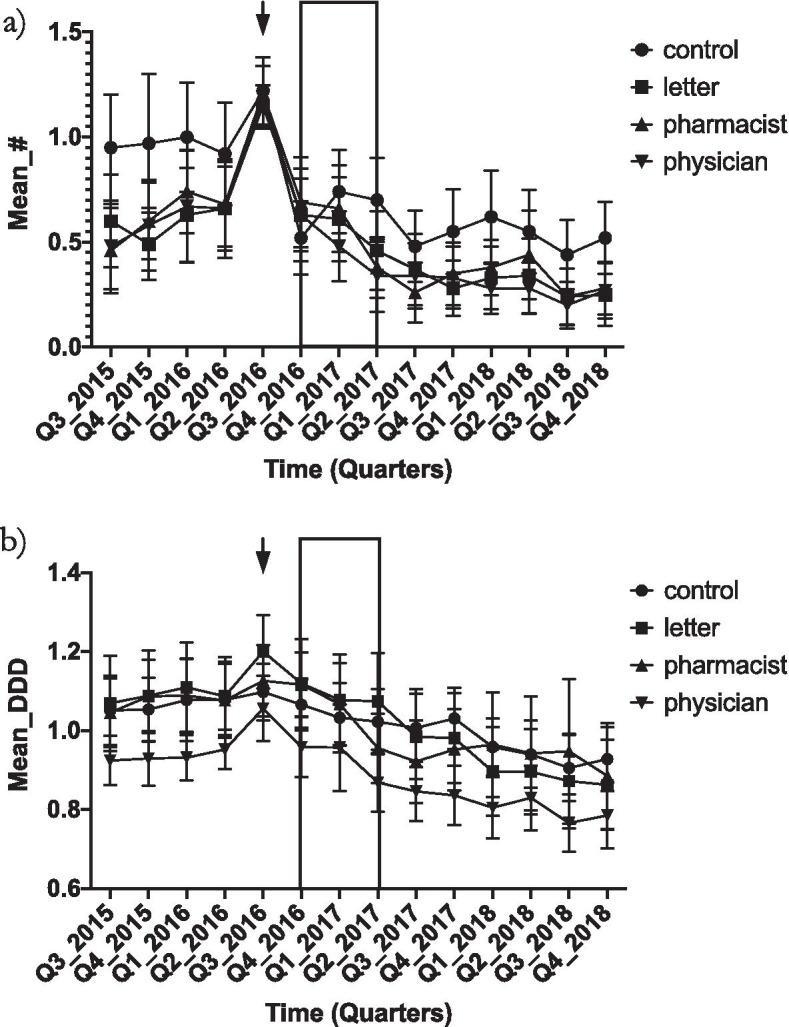
Methods: This was a four-armed, one year, blinded, randomized, parallel-group, investigational trial in Alberta, Canada. Participants were fully licensed physicians (n = 272) who had prescribed 4 times the defined daily dose (4 + DDD) or more of any BDZ + to an older patient at least once in the 3rd quarter of 2016. All physician-participants were sent a personalized prescribing profile by the MRA. They were then randomized into four groups that received either nothing more, an additional personal warning letter from the MRA, a personal phone call from an MRA pharmacist or a personal phone call from an MRA physician. The main outcomes were prescribing behavior change of physicians at one year in terms of: change in mean number of older patients receiving 4 + DDD BDZ + and mean dose BDZ + prescribed per physician. To adjust for multiple statistical testing, we used MANCOVA to test both main outcome measures simultaneously by group whilst controlling for any baseline differences.
Results: All groups experienced a significant fall in the total number of older patients receiving 4 + DDD of BDZ + by about 50% (range 43-54%) per physician at one year, and a fall in the mean dose of BDZ + prescribed of about 13% (range 10-16%). However, there was no significant difference between each group.
Conclusions: A personalized prescribing report alone sent from the MRA appears to be an effective intervention for reducing very high levels of BDZ + prescribing in older patients. Additional interventions by a pharmacist or physician did not result in additional benefit. The intervention needs to be tested further on a more general population of physicians, prescribing less extreme doses of BDZ + and that looks at more clinical and healthcare utilization outcomes.
Keywords: Benzodiazepines; Interventions; Physicians; Prescribing.
Conflict of interest statement
None for any authors. The views and comments expressed in this article are solely the views of the authors and do not necessarily reflect the views of the College of Physicians and Surgeons of Alberta nor the University of Alberta.
Figures
References
-
- Special Advisory Committee on the Epidemic of Opioid Overdoses. National report: Apparent opioid-related deaths in Canada (January 2016 to December 2017) Ottawa: Public Health Agency of Canada; 2018 June.
-
- International Narcotic Control Board. Narcotic drugs technical report: estimated world requirements for 2017 – statistics for 2015.: United Nations; 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
